SEARCH
 = Registered users
= Registered users = Paid-up subscribers
= Paid-up subscribersPreset searches
PubMed -Respiratory medicine
Obstructive sleep apnoea hypopnoea
Tuberculosis primary care review
Upper respiratory tract infections
Lower respiratory tract infections
Cullinan P, Cannon J. Occupational asthma often goes unrecognised. Practitioner 2012;256 (1756):15-18
Occupational asthma often goes unrecognised
12 Dec 2012
AUTHORS
Professor Paul Cullinan MD FRCP, Professor in Occupational and Environmental Respiratory Disease
Ms Julie Cannon RGN RMN, Clinical Nurse Specialist, Royal Brompton Hospital, London, UK
Article
Abstract
Occupational asthma is induced de novo by an airborne agent encountered in the workplace. The risk of occupational asthma is greater in those with a prior atopic history. Work-exacerbated asthma is the provocation of pre-existing, or coincidental, disease by one or more irritant exposures at work. Distinguishing occupational from work-exacerbated asthma can be difficult but it is important since the two have very different clinical, occupational and legal implications. Occupational asthma is underrecognised, the disease often develops in young people who are otherwise fit. They may not recognise their symptoms as anything out of the ordinary, or may confuse them with hay fever or a cold. It is sensible to consider occupational and work-exacerbated asthma in every working adult who has asthma or who presents with suggestive symptoms such as rhinitis. Occupational asthma almost always arises from an immediate-type hypersensitivity reaction to a respiratory sensitising agent in the workplace. The disease has a short latency with symptoms developing 6 to 36 months after employment in a new job. Rhinitis is common and in those working in an environment with airborne proteins the absence of rhinitis effectively rules out occupational asthma. In occupational asthma, symptoms (including nasal symptoms) improve away from work. Once the disease is established symptoms are provoked by even very small exposures at work and begin to be provoked by a wide variety of irritant exposures both at, and away from, work. It is good practice to enquire into the employment of every working-age adult with asthma, or rhinitis, and particularly in those presenting with new symptoms or symptoms that have become more difficult to manage. Patients should routinely be asked whether their symptoms improve when they are not at work.
Consider these two narratives:
1 ‘I never had asthma until I started this job; if I hadn’t done this job then I wouldn’t have this asthma.’
2 ‘I’ve had asthma since I was a child; working in this job makes it worse.’
The first describes occupational asthma, a disease that is induced de novo by an airborne agent encountered in the workplace.1 In the description above it has arisen without a previous history but there is no reason, of course, why occupational asthma cannot develop in an individual with constitutional asthma. Indeed for many workplace agents the risk of occupational asthma is greater in those with a prior atopic history.
The second narrative is that of work-exacerbated asthma, the provocation of pre-existing or coincidental disease by one or more irritant exposures at work. Such exposures are legion, and include a large variety of volatile chemicals, airborne dusts and fumes, cold air, physical exertion and even early morning shift patterns. Most people with asthma have little trouble at work; when they do it is generally a reflection of inadequately treated disease.
Distinguishing occupational from work-exacerbated asthma can be difficult but it is important since the two have very different clinical, occupational and legal implications.
Common culprits
Around 400 separate agents encountered at work have been reported as causes of occupational asthma. Fortunately, most cases recognised in the UK arise from just a dozen of these, listed in box 1. Clinicians who look after people with asthma should have such a list to hand but it is important to bear in mind that it is not exhaustive.
There is little doubt that occupational asthma is underrecognised. There are several reasons for this:
• The disease often develops in young people who are otherwise fit. They may not recognise their symptoms as anything out of the ordinary, or may confuse them with other more common ailments such as hay fever or a cold
• People who have symptoms that they relate to their work may not wish to raise them with a doctor for fear of losing their employment or may simply accept them as part of the job
• Doctors in both primary and secondary care are notoriously poor at recognising occupational asthma
In an Oxfordshire general practice with 9,000 registered patients, there were 346 adults of working age with asthma. Around half of these, 182, had adult-onset disease, a third of whom were working in a job with a high risk of occupational asthma. Seven (4%) were recognised as having occupational asthma, a figure which probably underestimates the true proportion by about a half.
The authors of this study remarked that ‘the diversity of employment in our study area makes it difficult for the GP to remember every possible association.’2
Assessing patients
It is sensible to consider occupational and work-exacerbated asthma in every working adult who has asthma or who presents with suggestive symptoms. The same is true for those with rhinitis since this is a common accompaniment and precursor of occupational asthma, see figure 2.
While the risks — and thus the prior probability — of disease are greater in those with high-risk occupations it is worthwhile carrying out a simple screen of everyone in work.
Occupational asthma almost always arises from an immediate-type hypersensitivity allergic reaction to a respiratory sensitising agent in the workplace. The clinical picture reflects this process:
• Typically, the disease has a short latency with symptoms developing between 6 and 36 months after employment in a new job
• The latency is important; symptoms that develop immediately after new employment are seldom those of occupational asthma – and more probably of the work-exacerbated type
• Rhinitis is common; indeed in those working in an environment with airborne proteins (bakers, animal workers, food processors) the absence of rhinitis effectively rules out occupational asthma
• When they are present, the symptoms of rhinitis commonly precede those of asthma. In the early stages of their disease, patients with occupational asthma will often complain that they have developed hay fever or say that ‘ever since I started this job I’ve had a cold.’
• In occupational asthma, symptoms (including nasal symptoms) improve away from work. In the early stages
of the disease this improvement is rapid — overnight. However, as time passes, with continuing exposure to the causative agent, the rate of improvement slows and symptoms resolve only after several days or even weeks away from work. Eventually there may be no improvement at all
• Because the disease is reflective of a hypersensitivity, once it is established symptoms are provoked by even very small exposures at work; herein lies the chief difficulty in managing occupational asthma
• Once the disease is established, patients tend to have more or less persistent bronchial hyperreactivity. Many will then find that their symptoms begin to be provoked by a wide variety of irritant exposures both at and away from work; this is a common source of diagnostic error and confusion with work-exacerbated asthma. It is also the reason why many patients with occupational asthma will, usually wrongly, attribute their symptoms to workplace agents that have a powerful odour.
Bearing these features in mind, it is good practice to enquire into the employment of every working-age adult with asthma, or rhinitis, and particularly in those presenting with new symptoms or with symptoms that have become more difficult than usual to manage. An appropriate question should be included in each asthma review to accommodate changes in employment. A job title or employer name is usually insufficient.
Those who are in work should routinely be asked whether their symptoms improve when they are not at work. This is a more specific question than asking: ‘Are your symptoms worse at work?’ In those who report improvement away from work, a careful history into the timing and development of their symptoms in relation to any change in employment (or in their tasks or exposures at work) will usually be illuminating.
Warning signals for occupational asthma are shown in box 2, above.
Implications of occupational asthma
Most patients with occupational asthma have to change their work. This is because continuing exposure to the causative agent carries a significant risk of developing intractable disease; and because the condition is one of hypersensitivity, reductions in exposure that are sufficient to eliminate symptoms and airway inflammation are rarely attainable without complete avoidance. The use of respiratory protection face masks, for example, is seldom effective even if desirable.
Moreover, the diagnosis carries important statutory and legal implications for an employer. The costs to all parties can be high.
Confirming diagnosis
For these reasons, it is important to get the diagnosis right. A false-positive diagnosis of occupational asthma is generally disastrous while missing a case risks at best an ever-increasing reliance on medications with diminishing returns, and at worst a missed opportunity to prevent irreversible asthma.
The British Thoracic Society recommends that every patient in whom the diagnosis is suspected is referred to a respiratory specialist with an interest in occupational lung disease. A list of these is available at http://www.hsl.gov.uk/centres-of-excellence/centre-for-workplace-health/gords/contact-information.aspx It is seldom necessary, and generally unhelpful, to recommend that a patient stay away from work while investigations are underway; the exceptions are those few who are clearly made very ill by being at work. Before making a referral, it is important to be sure that the patient is aware of the potential implications of a positive diagnosis.
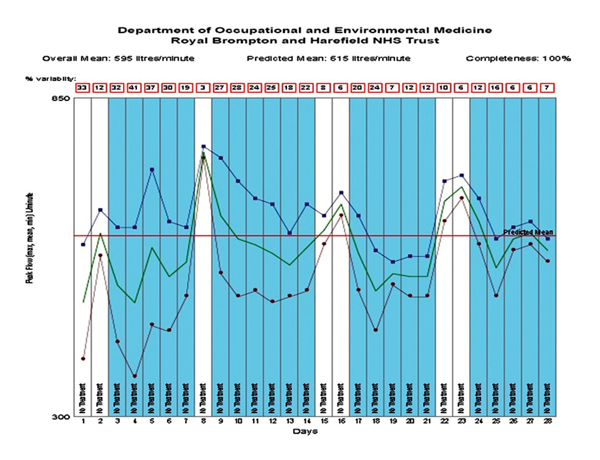
Specialist investigations will include immunological tests of specific sensitisation and functional tests of an asthma-work relationship, usually through serial measurement of peak flow, at least four times a day, preferably more, for at least a month, see figure 1, p15.
Note that twice daily measurements are very insensitive and that the interpretation of peak flow records in this respect requires considerable experience. In around 15% of cases patients require admission to hospital for specific provocation testing under carefully controlled conditions with the suspect agent.
Management options
The patient with occupational asthma faces a difficult dilemma. Continuing exposure will almost certainly result in persisting symptoms that will become increasingly difficult to manage pharmacologically with the risk that in time they will become irreversible. The avoidance of exposure usually requires a change in job, an unwelcome prospect for most people. Decisions do not need to be made immediately and offering a period for reflection and adjustment, of up to 2-3 months, is a kindness.
In most cases the decisions are effectively made by the employer, assuming that they are made aware of the diagnosis. If the organisation is large — and sympathetic — then redeployment may be offered. This is seldom possible in small firms and impossible, of course, for those who are self-employed. Where there is one, liaison with the relevant occupational health service is strongly recommended and usually very helpful.
Some patients, often those who work for themselves or those who do not wish their employers to know of their diagnosis, may choose to continue in the same work. They need to know the risk that this entails and to be offered suitable advice in relation
to protection at work and the appropriate use of standard asthma and allergy treatments. Specific immunotherapy is not used for occupational allergies in the UK.
Follow-up
Patients with occupational asthma who subsequently, in one way or another, avoid exposure should be followed up to assess any consequent improvement in their disease and to adjust any treatment they are taking. This may take up to two years but is a process that can generally be done in primary care.
In most cases an optimistic prognosis can be offered; indeed many patients feel enormously better once they are no longer exposed to the cause of their symptoms.
Those who choose to continue in exposure need regular review with the opportunity to reconsider their decision.
Employees with occupational asthma, whether or not they remain in (the same) employment, are eligible to make a claim for Industrial Injuries Disablement Benefit. The benefit is not available to the self-employed.
REFERENCES
1 Nicholson PJ, Cullinan P, Burge PS, Boyle C. Occupational asthma: Prevention, identification, and management: Systematic review and recommendations. BOHRF. London. 2010
2 de Bono J, Hudsmith L. Occupational asthma: a community based study. Occup Med (Lond). 1999;49 (4):217-9
ARTICLE IN PDF
EXTERNAL WEBLINKS
British Occupational Health Research Foundation
Free guidance on all aspects of occupational asthma; and on broader topics related to asthma and employment
Lungs at Work
Department of Occupational and Environmental Medicine at Royal Brompton Hospital, London: clinical advice, referrals, training
Occupational lung disease specialists
List of UK respiratory specialists with an interest in occupational lung diseases
The British guideline on asthma management. SIGN 153
Last revised 2016
Asthma: diagnosis, monitoring and chronic asthma management NICE NG80
In November 2017 NICE published the above guideline on diagnosing, monitoring and managing asthma in adults, young people and children. It does NOT cover managing severe asthma or acute asthma attacks.
Putting NICE NG80 guideline into practice in the UK
NICE recommends objective testing with spirometry and FeNO for most people with suspected asthma. Additional infrastructure and training is needed in primary care. In the meantime, NICE say primary care services should implement what they can of NG80 guideline, using currently available approaches to diagnosis.
Asthma UK professional resources
Videos to talk through inhaler technique with patients
Action plans for adults
Action plans for children
Non-English action plans
Filling in an asthma plan with a patient
Asthma review with a patient