SEARCH
 = Registered users
= Registered users = Paid-up subscribers
= Paid-up subscribersHannon É, Maxwell AP. Prompt investigation improves outcomes for kidney cancer. Practitioner Feb 2018;262(1812):17-20
Prompt investigation improves outcomes for kidney cancer
22 Feb 2018
AUTHORS
Dr Éadaoin Hannon MBChB MRCP, Specialist Registrar in Nephrology
Professor Alexander P. Maxwell, Consultant Nephrologist
Regional Nephrology Unit, Belfast City Hospital, Belfast, UK
Competing interests: None
Article
Kidney cancer is the seventh most common cancer in the UK, accounting for 3% of all new cases in 2015. Incidence rates for kidney cancer are projected to rise by 26% between 2014 and 2035, to 32 cases per 100,000 people per annum. Renal cell carcinoma (RCC) accounts for 80% of kidney cancers, of which clear cell (ccRCC) is the main subtype. There is a male preponderance in a ratio of 3:2. Smoking, obesity and hypertension are common risk factors and all three demonstrate a dose-response relationship with the relative risk of RCC. Malignant cyst formation may occur in chronic renal failure patients with acquired kidney cyst disease. There is a two-fold increase in risk of RCC in those with an affected first-degree relative, and 2-3% of RCC cases are due to a recognised hereditary syndrome. More than half of RCCs are detected incidentally on radiological imaging reflecting its often occult presentation. Nevertheless, it is recognised that a GP referral is the most common route to diagnosing kidney cancer. RCC should be suspected in the presence of: localising symptoms such as flank pain, a loin mass or haematuria; constitutional upset including weight loss, pyrexia and/or night sweats; or unexplained test results. Between 25 and 31% of individuals with kidney cancer will have metastatic disease at diagnosis and may present with dyspnoea, persistent cough, haemoptysis, bone pain, pathological fracture or lymphadenopathy.
Kidney cancer is the seventh most common cancer in the UK, accounting for 3% of all new cases in 2015.1
Incidence rates for kidney cancer are projected to rise by 26% between 2014 and 2035, to 32 cases per 100,000 people per annum.2 This prediction reflects both an ageing population, 50% of new kidney cancer cases in the UK are diagnosed in people aged 70 and over,1 and the rising prevalence of obesity, a recognised risk factor for cancer.
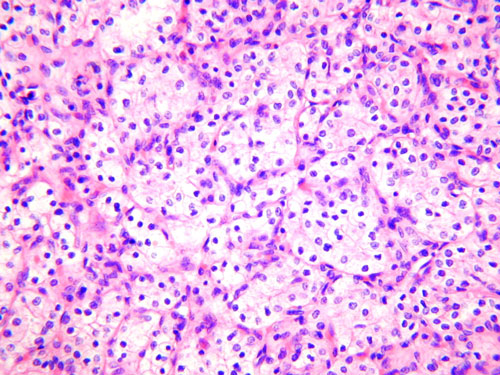
Renal cell carcinoma (RCC) is the focus of this article and accounts for 80% of kidney cancers, of which clear cell (ccRCC), see figure 1, is the main subtype (around 75%).1,3 There is a male preponderance in a ratio of 3:2.4
The diagnosis of kidney cancer can be challenging because of its varied and non-specific symptoms and limited early warning signs. More than half of RCCs are detected incidentally3,4 on radiological imaging reflecting its often occult presentation.
Nevertheless, it is recognised that a GP referral is the most common route to diagnosing kidney cancer.1 With a high level of clinical suspicion and prompt investigation, kidney cancer can be diagnosed at an early stage and this is associated with improved survival. More than 8 in 10 patients with an early stage diagnosis will survive their disease for at least five years but this falls to 1 in 10 for patients with late stage kidney cancer at diagnosis.1
Clinical features
Primary care consultation may be triggered by one of the varied presentations outlined in table 1.
RCC should be suspected in the presence of:
• Localising symptoms such as flank pain, a loin mass or haematuria
• Constitutional upset including weight loss, pyrexia and/or night sweats
• Unexplained laboratory test results
Abnormal test results in a symptomatic patient may include anaemia and a raised ESR or C-reactive protein in the absence of infection. Paraneoplastic syndromes are found in approximately 30% of patients with symptomatic RCC4 and are caused by secretion of tumour-derived hormones. These syndromes can be associated with polycythaemia (erythropoietin), hypercalcaemia (parathyroid hormone related peptide) or hypertension (renin).
Between 25 and 31% of individuals with kidney cancer will have metastatic disease at diagnosis1 and may present with dyspnoea, persistent cough, haemoptysis, bone pain, pathological fracture or lymphadenopathy. Local tumour spread into the left renal vein may result in a non-reducing varicocoele and extensive tumour involvement within the inferior vena cava may cause bilateral leg oedema.5,6
Risk factors
Lifestyle
Recognised risk factors exist for RCC, see table 2. Smoking, obesity and hypertension are common risk factors and all three demonstrate a dose-response relationship with the relative risk of RCC.7,8,9 These risk factors are potentially modifiable and can be targeted in primary care and through public health promotion. Protective lifestyle factors include physical activity, moderate alcohol intake and consumption of cruciferous (cabbage-like) vegetables.4
Environmental
RCC is not a typical occupational disease10 however exposure to trichloroethylene (metal degreaser) has been implicated. Aniline dyes, used in textile, rubber and plastic industries predispose to renal pelvis transitional cell carcinomas rather than RCCs.
Acquired cystic kidney disease (ACKD) occurs in chronic renal failure from any aetiology. Malignant cyst transformation is a recognised complication of ACKD with a 40-fold increased risk compared with the general population.11 Thus there should be a higher index of suspicion for RCC in chronic dialysis and renal transplant recipients who are at increased risk of RCC in their native kidneys. Inherited autosomal dominant polycystic kidney disease does not appear to be a risk factor for RCC.
Genetic
Around 2-3% of all RCC are due to a recognised hereditary syndrome. There is a two-fold increase in risk of RCC in those with an affected first-degree relative.10 Several hereditary renal cancer syndromes exist12 and those specific to ccRCC include: von Hippel-Lindau syndrome type 1/type 2B (retinal, central nervous system and renal tumours); tuberous sclerosis complex (developmental delay, epilepsy with central nervous system, skin and renal hamartomas); and familial ccRCC for which the genetic mutation is unknown.6
These syndromes have an autosomal dominant inheritance pattern and family members at risk should be counselled to consider relevant clinical and genetic testing.10,12
Investigations
Ultrasound is a useful initial screening tool when clinical suspicion of RCC is high (e.g. loin pain, flank mass, haematuria or constitutional symptoms). This should be arranged as a red flag investigation. During a consultation other useful simple tests include a urinalysis, full blood picture, ESR, bone profile, liver function tests and an electrolyte profile.
As a test, urinalysis can be of value in unravelling the possible aetiology of visible and non-visible haematuria. Urinary tract infection (UTI) is suggested by the coexistence of leukocytes ± nitrites on dipstick testing. The presence of coexisting proteinuria may suggest an intrinsic renal glomerular pathology. A spot albumin: creatinine ratio will quantify any proteinuria in this setting. However, importantly, haematuria in the absence of co-existing proteinuria suggests a possible underlying structural abnormality in the kidneys, ureters or bladder that may need further evaluation through ultrasound and cystoscopy.
Visible haematuria should trigger suspicion for urological malignancy. Prostate and bladder malignancy are outside the scope of this article. NICE has updated guidance on referral to secondary care for suspected renal and bladder cancers, summarised in table 3, opposite. It is recommended that patients aged 45 years and over with visible haematuria that is unexplained, present in the absence of UTI or persists/recurs after treatment of UTI should be referred urgently for an appointment within two weeks.13 However, younger patients can have earlier onset of disease. Clinicians should always exercise their own clinical judgement when deciding which patients to refer.
CT or MR imaging will be undertaken in secondary care following an initial abnormal ultrasound. This gives useful information on tumour extension locally, the appearance of the contralateral kidney and aids staging through identification of metastases.4
Treatment
Surgery
For localised (kidney-limited) disease, particularly when tumour size is < 7 cm, there has been a move toward nephron sparing surgery in the form of partial nephrectomy, however, tumour position in the kidney along with patient choice and consideration of comorbidity will dictate the suitability of such a procedure.4,6,14
If feasible, nephron sparing surgery is also preferred for management of hereditary RCC due to increased risk of future tumours. For more advanced RCC staging with localised invasion of adjacent structure (adrenal tissue, vena cava below diaphragm and not beyond Gerota’s fascia) radical nephrectomy remains the best option for an attempt at curative therapy. Following surgical resection, 20-30% will experience a relapse often in the form of pulmonary metastases14 and therefore active interval radiological surveillance is required.
Other options include radiofrequency ablation and cryoablation which may be preferable for renal cortical tumours < 3-5 cm; where there is a solitary kidney or chronic kidney disease; known hereditary/bilateral RCC; or in frail patients unfit for surgery.3,6
Sometimes interval surveillance (watchful waiting) may be deemed appropriate if the tumour is small and growing slowly. Embolisation for symptom control (haematuria and/or pain) can be undertaken in those unfit for surgery or with non-resectable cancer.4
Targeted systemic therapy and immunotherapy
Targeted systemic therapy modulates molecular pathways that typically promote tumour growth. In ccRCC it is recognised that a mutation results in the production of cytokines stimulating angiogenesis. Tyrosine kinase inhibitors (TKIs) inhibit vascular endothelial growth factor (VEGF) and platelet-derived growth factor (PDGF) which in turn prevents tumour cell proliferation and development of tumour blood vessels. The TKIs sunitinib, pazopanib, and sorafenib are currently approved by NICE for treatment of advanced and metastatic RCC.16,17 In 2015, NICE recommended a multitargeted TKI inhibitor, axitinib, for treatment in advanced RCC after failure of prior systemic treatment.18 Temsirolimus and everolimus are mammalian target of rapamycin (mTOR) inhibitors that can be used in the management of advanced RCC. mTOR inhibitors prevent tumour cell division and blood vessel growth in tumours.
Immunotherapy triggers an immune response that destroys the cancer cells. Monoclonal antibodies directed at VEGF are used in the treatment of advanced/metastatic RCC. Bevacizumab received NICE approval in 200916 but is no longer recommended as a first-line treatment. Nivolumab, a fully human antibody that blocks ligand activation of the programmed death receptor 1 (PD-1) restores cellular immunity and is the only treatment that has shown overall survival benefit in patients who have been previously treated for advanced RCC.15 NICE published guidance on this therapy in 2016.19
Therapeutic options continue to expand and the selection of an appropriate treatment plan is often individualised to the patient taking into account comorbidity, functional status, stage and rate of tumour progression. Patients in receipt of these therapies do experience toxicity and may present to primary care. Common toxicities relating to the TKIs include rash, diarrhoea, mucositis, hand-foot syndrome, thyroid dysfunction, hypertension and left ventricular dysfunction and blood dyscrasias.
Conclusion
The incidence of kidney cancer is rising with a lifetime risk of 1 in 52 for men and 1 in 87 for women.1 GPs will therefore encounter kidney cancer quite frequently and by maintaining a high index of clinical suspicion can help to ensure a prompt diagnosis is made. Improved survival is related to earlier disease recognition and less advanced staging at presentation.
Unexplained visible haematuria in patients over 45 years should trigger referral for suspected renal cancer, as per NICE guidance. For the subtler presentations of RCC, basic blood and urine testing, in conjunction with ultrasound, can provide the necessary information to guide secondary care referral.
The range of treatments, both surgical and systemic, is expanding and requires a coordinated approach between primary and secondary care. Therefore, fundamental knowledge on current treatment options, potential therapy toxicities and indeed where to source information (see Useful information box) is essential in supporting patients as they navigate an often uncertain journey following diagnosis.
REFERENCES
1 Cancer Research UK. Kidney Cancer Statistics. http://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/kidney-cancer#heading-Zero Last accessed 24 January 2018
2 Smittenaar CR, Petersen KA, Stewart K, Moitt N. Cancer incidence and mortality projections in the UK until 2035. Br J Cancer 2016;15(9):1147-55
3 Escudier B, Porta C, Schmidinger M et al. Renal cell carcinoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol 2016;27 (Supplement 5): v58–v68, doi:10.1093/annonc/mdw328
4 European Association of Urology. Renal Cell Carcinoma update March 2016. https://uroweb.org/wp-content/uploads/EAU-Guidelines-Renal-Cell-Carcinoma-2016.pdf Last accessed 24 January 2018
5 El Abiad Y, Qarro A. Acute varicocele revealing renal cancer. N Engl J Med 2016;374:2075 DOI: 10.1056/NEJMicm1506668
6 British Association of Urological Surgeons and British Uro-oncology Group. Multi-disciplinary Team (MDT) Guidance for Managing Renal Cancer. May 2012 www.baus.org.uk/userfiles/pages/files/Publications/MDTRenalCancerGuidance.pdf
7 Bergström A, Hsieh CC, Lindblad P et al. Obesity and renal cell cancer – a quantitative review. Br J Cancer 2001;85(7):984-990
8 Wong-Ho C, Dong LM, Devesa SS. Epidemiology and risk factors for kidney cancer. Nat Rev Urol 2010;7(5): 245-57
9 Weikert S, Boeing H, Pischon T et al. Blood pressure and risk of renal cell carcinoma in the European prospective investigation into cancer and nutrition. Am J Epidemiol 2008;167:438-46
10 Ljungberg B, Campbell SC, Cho HY et al. The epidemiology of renal cell carcinoma. Eur Urol 2011;60:615-621
11 Foshat M, Eyzaguirre E. Acquired cystic disease-associated renal cell carcinoma: Review of pathogenesis, morphology, ancillary tests, and clinical features. Arch Pathol Lab Med 2017;141(4):600-06
12 Morrison PJ, Donnelly DE, Atkinson AB, Maxwell AP. Advances in the genetics of familial renal cancer. Oncologist 2010;15:532-38
13 National Institute for Health and Care Excellence. NG12. Suspected cancer: Recognition and referral. NICE. London. 2015 (updated July 2017)
14 Motzer RJ, Jonasch E, Agarwal N et al. Kidney Cancer, Version 2.2017, NCCN Clinical Practical Guidelines in Oncology. J Natl Compr Canc Netw 2017;15:804-34
15 National Cancer Institute. Renal Cell Cancer Treatment (PDQ®) – Health professional version. Published 19 Jan 2018 Accessed at: www.ncbi.nlm.nih.gov/books/NBK65815/ Last accessed 25 January 2018
16 National Institute for Health and Care Excellence. TA178. Bevacizumab (first-line), sorafenib (first- and second-line), sunitinib (second-line) and temsirolimus (first-line) for the treatment of advanced and/or metastatic renal cell carcinoma. NICE. London. 2009
17 National Institute for Health and Care Excellence. TA215. Pazopanib for the first-line treatment of advanced renal cell carcinoma. NICE. London. 2011
18 National Institute for Health and Care Excellence. TA333. Axitinib for treating advanced renal cell carcinoma after failure of prior systemic treatment. NICE. London. 2015
19 National Institute for Health and Care Excellence. TA417. Nivolumab for previously treated advanced renal cell carcinoma. NICE. London. 2016
ARTICLE IN PDF
PRESET SEARCHES
PubMed
US NCI
NICE evidence search
EXTERNAL WEBLINKS
Patient information including links to clinical trials
Understanding kidney cancer booklet and patient helpline
Patient information about kidney cancer
Patient website