SEARCH
 = Registered users
= Registered users = Paid-up subscribers
= Paid-up subscribersHopper AD, Campbell JA. Improving outcomes in pancreatic cancer. Practitioner July/Aug 2018;262(1817):11-15
Improving outcomes in pancreatic cancer
25 Jul 2018
AUTHORS
Dr Andrew D Hopper MD FRCP, Gastroenterology Consultant
Dr Jennifer A Campbell MD MRCP, Clinical Fellow in Gastroenterology
Department of Gastroenterology, Royal Hallamshire Hospital, Sheffield, UK
Article
Abstract
Pancreatic ductal adenocarcinoma has a very poor prognosis. The five-year survival rate for pancreatic cancer is 3% in the UK. There has been very little improvement in outcomes over the past 40 years. The combination of an aggressive disease, vague presenting symptoms and insensitive standard diagnostic tests is a key factor contributing to poor outcomes with only 15% of patients with pancreatic cancer having operable disease at diagnosis. Although pancreatic cancer has a peak incidence in the ninth decade, 37% of patients are under 70 and 14% are under 60 years of age. In patients aged 60 and above, jaundice has a positive predictive value (PPV) of 22%, whereas other symptoms, such as abdominal pain, altered bowel habit or new onset diabetes, are non-specific with a PPV of less than 1%. However, associated weight loss increases the PPV to between 1.5 and 2.7%. The NICE guideline on referral for suspected cancer recommends urgent referral via a suspected cancer pathway referral if the patient is aged 40 and over with jaundice. It also recommends that an urgent direct access computerised tomography (CT) scan referral should be considered in patients aged 60 and over with weight loss and any of the following: diarrhoea; back pain; abdominal pain; nausea; vomiting; constipation; new onset diabetes. Pancreatic cancer requires a CT scan for diagnosis. Although trans-abdominal ultrasound is excellent at detecting gallstones and confirming obstructive jaundice by the presence of bile duct dilatation, the presence of gas in the stomach makes visualisation of the pancreas poor.
Pancreatic ductal adenocarcinoma has a very poor prognosis. The current five-year survival rate for pancreatic cancer is 3% in the UK. There were 9,921 patients diagnosed with pancreatic cancer in the UK in 2015 and almost an equal number of patients (9,263) dying from the disease in 2016.1
There has been little improvement in outcomes for this disease in the past 40 years.2 Pancreatic cancer is the eleventh most common cancer in the UK. However, its poor outcomes make it the fifth most common cause of cancer deaths.1 The incidence of pancreatic cancer is increasing by 2% per year and when coupled with its poor outcomes and treatment for other cancers becoming more effective means that pancreatic cancer is likely to supersede breast cancer as at least the fourth most common cause of cancer deaths in the UK by 2035.3 Relative survival rates for pancreatic cancer in the UK are lower than the average for Europe.2
The combination of an aggressive disease, vague presenting symptoms and poor sensitivity of standard diagnostic tests is a key factor contributing to poor outcomes with only 15% of patients with pancreatic cancer having operable disease at diagnosis. This article focuses on the recognition of symptoms and risk factors that can aid early referral, diagnosis and treatment to improve outcomes for a disease that has such a relatively short survival compared with other cancers that it has been referred to as a medical emergency.4
In February 2018, NICE published a clinical guideline on pancreatic cancer in adults (NG85) to help improve early detection and management.5
Presentation
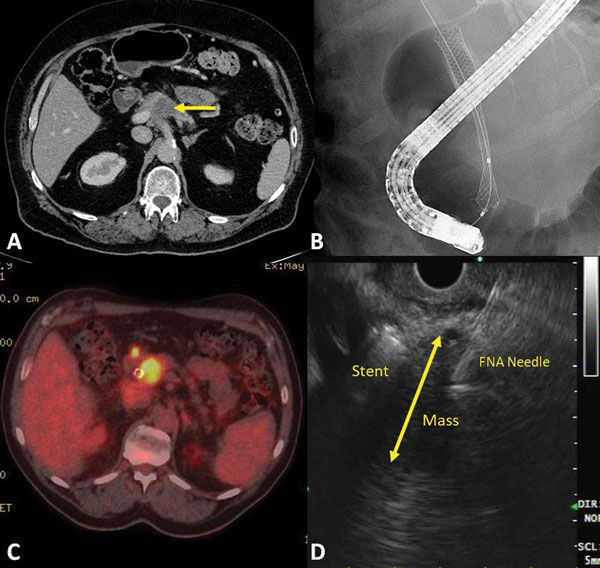
Diagnosis at an early stage is associated with improved survival therefore it is important to note the high-risk symptoms that require investigation. Patients may present with symptoms of local compression or invasion of mesenteric nerves or the bile duct (see figure 1), changes in bowel habit caused by alterations in exocrine pancreatic function and new onset diabetes. There have been a number of studies looking at symptom presentation of pancreatic cancer and the increased risk associated with each one.6
The recommendations for urgent referral for suspected pancreatic cancer listed in the NICE guideline NG12. Suspected cancer: recognition and referral, are shown in table 1.
Jaundice, with or without pain, has been shown to have a positive predictive value (PPV) of 22% in patients aged ≥ 60 and although other symptoms listed have been shown to have a PPV of < 1% as a single symptom, when combined with weight loss in patients over 60 this increases to 1.5-2.7%.7
Although pancreatic cancer has a peak incidence in patients in their ninth decade,8 37% of patients present under the age of 70 and 14% are under 60, therefore some cancer charities promote consideration of urgent referral or investigation in all patients over 40 with unexplained symptoms not just those who are jaundiced (see table 2). This practice is more in keeping with a GP’s gut feeling which has been shown to be a strong predictor of pancreatic cancer in one Danish study (PPV = 22.5%) highlighting the need for direct access computerised tomography (CT).9
A rarer neuroendocrine type of pancreatic tumour exists which can have a more benign course. Neuroendocrine tumours account for only 1.5% of all pancreatic cancers and are often found incidentally or secrete certain hormones. Their complex management is outside the scope of this article which refers to pancreatic cancer as the ductal adenocarcinoma type.10
Examination and assessment
It has been shown that nearly a third (31.4%) of patients present to their GP at least three times before a diagnostic test is carried out or a referral is made.10
A full-time GP would only be expected to see one case of pancreatic cancer in five years,7 therefore it is important to note the high-risk symptoms that necessitate investigation and referral. Unfortunately, current urgent cancer referral pathways have a poor sensitivity and only detect 15% of pancreatic cancers. A significant number of patients with pancreatic cancer present with worsening symptoms of vomiting from duodenal compression or jaundice which results in 50% of patients being diagnosed via an accident and emergency presentation.11,12
Given the position of the pancreas (see figure 1), it is difficult to detect a pancreatic mass on examination.
A detailed history of any weight loss (rather than BMI), developing chronic abdominal pains, obstructive projectile vomiting or persistent nausea and clinical detection of jaundice requires urgent investigation and exclusion of differential diagnoses, see table 3.
Confirming diagnosis
Pancreatic cancer requires a CT scan for diagnosis (see figure 1). There are a number of symptoms in patients when either direct access CT scan is suggested or urgent referral if not available.
Trans-abdominal ultrasound is excellent at detecting gallstones and bile duct dilatation to confirm obstructive jaundice, however the presence of gas in the stomach makes visualisation of the pancreas poor. NICE recommends an urgent ultrasound scan if CT is not available, see table 1.* However, although pancreatic abnormalities can be detected on ultrasound, especially in thin people, if the ultrasound scan is negative this should not deter urgent referral.
The differential diagnosis of symptoms can also meet the criteria for an urgent gastroscopy to exclude an upper gastrointestinal tumour or lesion and it is important to consider a CT and follow-up for patients with epigastric ‘dyspepsia’ that have either a normal gastroscopy or symptoms that have not responded to anti-acid therapy, see table 2.
Liver function blood tests should be performed to exclude or confirm jaundice. The serum tumour marker CA19-9 is not recommended for initial diagnostic assessment as levels can be significantly raised in obstructive jaundice from benign disease.13
CT has a high accuracy for staging and planning surgical resection.14 However, if the diagnosis is unclear or the tumour is not resectable then tissue sampling is required. This enables exclusion of atypical tumours to plan appropriate palliative chemotherapy.
Because of its location pancreatic tissue sampling is usually performed using endoscopic ultrasound (EUS) with fine needle aspiration (FNA). By passing an endoscope with a small ultrasound probe attached into the stomach and duodenum, the EUS probe is able to lie directly against the pancreas and sample abnormal areas.
Although the procedure has a low risk of complications (2.7%)15 the wider scope and the lengthy duration of the procedure requires the patient to be sedated.16 If liver metastases are present then a liver biopsy is an alternative option.
Risk factors
Modifiable pancreatic cancer risk factors include obesity and smoking. However, two-thirds of pancreatic cancer tumours are attributable to the random mutations that occur throughout an individual’s lifetime. There is an increased incidence of pancreatic cancer in a number of conditions including chronic pancreatitis (three fold) and hereditary pancreatitis (50 fold). 1,5 Surveillance for pancreatic cancer is currently recommended in hereditary pancreatitis, Peutz-Jeghers syndrome and patients with high-risk gene mutations who have a first-degree relative with pancreatic cancer.6 Annual MRI can be performed to look for early cancers, but given a lack of further evidence regarding the ideal timing of initiation or interval for screening it should be discussed and led by a secondary care specialist unit.5,17,18
Pancreatic cysts have been shown to account for a small proportion < 5% of pancreatic cancers. Although most cysts are benign or inflammatory, those containing mucin have malignant potential (termed either a mucinous cyst adenoma or intraductal papillary mucinous neoplasm).
The risk of a mucinous cyst becoming malignant is small (estimated at 0.72% per year).19 However if these cysts are removed before malignancy is detected outcomes are improved. Overall five-year survival after resection is 87% for all cystic lesions and 62% for those with malignancy.20
Pancreatic cysts are found incidentally on 2.6% of CT scans and given the increased uptake of cross-sectional imaging pancreatic cysts are becoming increasingly identified and potentially a cause of significant anxiety.21
Patients with a pancreatic cyst should be referred to secondary care for characterisation so that a decision can be made regarding further management, based on identified risk factors such as pancreatic duct enlargement.22,23
Management
Staging
Management options are discussed at a specialist pancreatic cancer multidisciplinary team (MDT) meeting involving specialist consultant surgeons, radiologists, pathologists, oncologists, gastroenterologists, palliative care physicians and also crucially attended by cancer nurse specialists and specialist dietitians. Investigation results are coupled with the patient’s fitness for surgery, chemotherapy and palliative options with the final decision made together with the patient after the clinician carefully explains the recommended treatment options.
Tumours are staged with a CT which is 80% accurate14 and additional information then gained from either a positron emission tomography (PET)-CT scan, MRI of the liver or an EUS and FNA if required (see figure 1) to enable tumour node metastasis (TNM) staging, see table 4. Clinically the TNM stage classifies patients into those with pancreatic cancer that are surgically resectable, locally advanced or metastatic. Only 15% of pancreatic cancers present at a resectable stage24 so management is predominantly palliative.
Curative surgery
Comorbidity plays a significant role when considering a surgical option as well as tumour size and proximity to vessels. Tumours in the head of the pancreas are removed with a Whipple’s procedure, for those in the body and tail a distal pancreatectomy is generally performed which usually removes the spleen as well. Pancreatic surgery is a significant undertaking as although the hospital mortality rates following surgery are below 2%, overall morbidity is up to 60%.25 As with most cancer centres, surgical outcomes for pancreatic cancer correlate with both numbers of cancers seen and operations performed with significantly lower mortality and morbidity at high volume centres. With the establishment of specialised cancer centres in the UK, the two-year survival among resected patients has increased by more than 10%.26 This association also applies to long-term survival and is multifactorial.27,28
Adjuvant chemotherapy is recommended after pancreatic cancer resection based on several randomised controlled trials which have shown that postoperative five year survival is increased from 8% to 21-23%.29,30
No definite advantage has been shown to recommend neoadjuvant therapy so therefore it is currently only considered for patients with resectable or borderline resectable pancreatic cancer in clinical trials.5
Palliative chemotherapy
First-line therapy for non-resectable pancreatic cancer in patients with a good performance status is usually gemcitabine increasing 12-month survival from 2 to 18%, however a significant response is seen in only 28% of patients31 therefore a combination regimen is recommend if patients are well enough to tolerate this.32
For metastatic pancreatic cancer a combination of oxaliplatin, irinotecan, fluorouracil, and leucovorin (FOLFIRINOX) has been shown to prolong survival from 6.8 months with gemcitabine alone to 11.1 months. However, this treatment does have significantly more adverse effects and therefore should only be considered in patients with a very good performance status.33 Lastly, albumin-bound paclitaxel (nab-paclitaxel) in combination with gemcitabine has been shown to give some benefit, mean survival 8.5 versus 6.7 months without.34
Biliary and duodenal obstruction
Jaundice is present in up to 70% of patients with pancreatic cancer. Jaundice causes lethargy, anorexia and intractable pruritus which is a distressing symptom. Biliary decompression and stenting can alleviate jaundice and symptoms, allowing bilirubin levels to fall and reducing the risk of toxicity during subsequent chemotherapy.35 Endoscopically placed self-expandable biliary metal stents show the best long-term results (see figure 1).36
Because of the higher rate of complications such as pancreatic fistulae and wound leakage biliary stents in resectable disease are currently avoided unless there is a delay to surgery, if the patient is too unwell, or a stent is required as part of a clinical trial.37 In patients with duodenal obstruction and difficult endoscopic access a percutaneous transhepatic approach can be performed to place a metal biliary stent.
The decision to proceed with biliary stenting should be discussed in the MDT meeting. Biliary stenting should not take place before an accurate pancreas protocol CT has been performed as the presence of a stent can significantly interfere with the ability of CT to stage pancreatic cancer.
Clinical and radiological evidence of duodenal obstruction requires treatment either with a radiologically placed metal duodenal stent (ideally in frail patients or in those with metastatic disease) or consideration of a gastric bypass for patients with a more favourable prognosis as duodenal stents can become blocked over time.38
Pain control
Pain affects approximately 80% of patients with pancreatic cancer, with half requiring stronger morphine-based drugs than codeine or tramadol. Pain is associated with poor survival, hazard ratio 1.61, as well as an impaired performance status and eligibility for chemotherapy.39,40 Side effects of opiates may limit their use. These include sedation, constipation, confusion, tolerance and dependence, which impact negatively on quality of life. Tricyclic antidepressants and gabapentin may be used as adjunctive treatments because of their neuromodulating properties.39
In refractory pain, EUS coeliac plexus neurolysis can be considered as it has been shown that a 60% greater reduction in pain scores can be achieved, compared with pharmacotherapy alone, at three months. Coeliac plexus neurolysis can also lower morphine requirements by 50% and although side effects of diarrhoea, orthostatic hypotension and pain can occur they usually resolve.41
Nutrition and malabsorption
Approximately 80% of patients with pancreatic cancer report weight loss at the time of diagnosis and more than a third have lost > 10% of their body weight through a combination of pain, jaundice, bowel obstruction and malabsorption.42 Specialist dietitian as well as cancer nurse support is essential to improve nutrition, function, and quality of life and also the ability to tolerate treatments.
Malabsorption because of pancreatic enzyme insufficiency occurs in more than 60% of patients with pancreatic cancer as a result of pancreatic invasion and obstruction of the pancreatic duct.43 A faecal elastase-1 test can be used to determine exocrine pancreatic function however given the poor sensitivity of the test and significant prevalence in unresectable cancer and after pancreatic resection (74% to 92%)43, 44 guidance has suggested that enzyme replacement therapy should be offered without relying on testing.5 The dose of enzyme needs to be titrated against symptoms and should be regularly reviewed. Proton pump inhibitors may be needed in some patients as they increase the efficacy of enzyme replacement by generating an alkaline environment in the duodenum in which enzymes are more physiologically active.
Depression
Up to 50% of patients with pancreatic cancer suffer from depression which in many develops before diagnosis.45,46 Biological effects of the cancer can alter the action and excretion of serotonin and lower mood further which in turn augments the effects of pain, anorexia, weight loss and psychological effects of receiving information on the diagnosis, treatments and prognosis.47 Therefore, early identification and treatment is essential although no particular antidepressant has been shown to be superior. If rapid access to psychological support is possible this should also be offered.
Diabetes
Pancreatic cancer can present with new onset diabetes or with existing type 2 diabetes worsening as the cancer progresses. Diabetes caused by loss of pancreatic function is termed type IIIc diabetes.48
More than half of pancreatic cancer patients have diabetes or hyperglycaemia, and the onset of diabetes typically occurs between 6 and 36 months before pancreatic cancer diagnosis in 20-25% of patients with pancreatic cancer.49 Uncontrolled diabetes can cause polydipsia, polyuria, lethargy and weight loss diminishing quality of life.
Metformin is the recommenced oral hypoglycaemic with the addition of insulin if required.50 However, metformin is contraindicated in patients with significant renal or hepatic impairment and must be stopped immediately before and after CT scanning in those with renal impairment.50
Conclusion
Pancreatic cancer currently has a very poor prognosis and diagnosis is often delayed. Improvements in early diagnosis are possible with raised awareness, prompt referral or the use of direct access CT that would increase the number of patients eligible for potentially curative surgery. Research to evaluate improvements in patient pathways to earlier surgery51 and individualised chemotherapy treatments by cancer DNA analysis are underway in the UK,52 however currently most patients present with advanced disease. Pancreatic cancer therefore requires early liaison between dietitians, cancer nurse specialists and primary, secondary and hospice care to enable access to support for patients and their families.
Competing interests: None
REFERENCES
1 Cancer Research UK. Pancreatic cancer statistics
[Last accessed 29 June 2018]
2 Cancer Research UK. Pancreatic cancer survival statistics. www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/pancreatic-cancer/survival#heading-Two [Last accesssed 29 June 2018]
3 Smittenaar CR, Petersen KA, Stewart K, Moitt N. Cancer incidence and mortality projections in the UK until 2035. Br J Cancer 2016;115:1147-55
4 Lohr JM. Pancreatic cancer should be treated as a medical emergency. BMJ 2014;349:g5261
5 National Institute for Health and Care Excellence. NG85. Pancreatic cancer in adults: diagnosis and management. NICE. London. 2018 www.nice.org.uk/guidance/ng85
[Last accessed 29 June 2018]
6 Becker AE, Hernandez YG, Frucht H, Lucas AL. Pancreatic ductal adenocarcinoma: risk factors, screening, and early detection. World J Gastroenterol 2014;20:11182-98
7 Stapley S, Peters TJ, Neal RD et al. The risk of pancreatic cancer in symptomatic patients in primary care: a large case-control study using electronic records. Br J Cancer 2012;106:1940-44
8 Cancer Research UK. Pancreatic cancer statistics. www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/pancreatic-cancer/incidence#heading-One [Last Accessed 29 June 2018]
9 Ingeman ML, Christensen MB, Flemming Bro F et al. The Danish cancer pathway for patients with serious non-specific symptoms and signs of cancer–a cross-sectional study of patient characteristics and cancer probability. BMC Cancer 2015;15:421
10 Halfdanarson TR, Rubin J, Farnell MB et al. Pancreatic endocrine neoplasms: epidemiology and prognosis of pancreatic endocrine tumors. Endocr Relat Cancer 2008;15:409-27
11 Lyratzopoulos G, Abel GA, McPhail S et al. Measures of promptness of cancer diagnosis in primary care: secondary analysis of national audit data on patients with 18 common and rarer cancers. Br J Cancer 2013;108:686-90
12 Pancreatic Cancer UK. Policy briefing: every life matters: the real cost of pancreatic cancer diagnoses via emergency admissions. www.pancreaticcancer.org.uk/media/450955/elm_policybriefing_final.pdf [Last accessed 29 June 2018]
13 Baghbanian M, Baghbanian A, Salmanroghani H, Shabazkhani B. Serum CA19-9 in patients with solid pancreatic mass. Gastroenterol Hepatol Bed Bench 2013;6:32-35
14 Karmazanovsky G, Fedorov V, Kubyshkin V, Kotchatkov A. Pancreatic head cancer: accuracy of CT in determination of resectability. Abdom Imaging 2005;30:488-500
15 Zhu H, Jiang F, Zhu J et al. Assessment of morbidity and mortality associated with endoscopic ultrasound-guided fine-needle aspiration for pancreatic cystic lesions: A systematic review and meta-analysis. Dig Endosc 2017;29:667-75
16 Campbell JA, Irvine AJ, Hopper AD. Endoscopic ultrasound sedation in the United Kingdom: Is life without propofol tolerable? World J Gastroenterol 2017;23:560-62
17 Signoretti M, Bruno MJ, Zerboni G et al. Results of surveillance in individuals at high-risk of pancreatic cancer: A systematic review and meta-analysis. United European Gastroenterol J 2018;6:489-99
18 Canto MI, Harinck F, Hruban RH et al. International Cancer of the Pancreas Screening (CAPS) Consortium summit on the management of patients with increased risk for familial pancreatic cancer. Gut 2013;62:339-47
19 Scheiman JM, Hwang JH, Moayyedi P. American Gastroenterological Association technical review on the diagnosis and management of asymptomatic neoplastic pancreatic cysts. Gastroenterology 2015;148:824-48 e22
20 Valsangkar NP, Morales-Oyarvide V, Thayer SP et al. 851 resected cystic tumors of the pancreas: a 33-year experience at the Massachusetts General Hospital. Surgery 2012;152:S4-12
21 Laffan TA, Horton KM, Klein AP et al. Prevalence of unsuspected pancreatic cysts on MDCT. AJR Am J Roentgenol 2008;191:802-07
22 European Study Group on Cystic Tumours of the Pancreas. European evidence-based guidelines on pancreatic cystic neoplasms. Gut 2018;67:789-804
23 Lennon AM, Ahuja N, Wolfgang CL. AGA Guidelines for the management of pancreatic cysts. Gastroenterology 2015;149:825
24 Ansari D, Gustafsson A, Andersson R. Update on the management of pancreatic cancer: surgery is not enough. World J Gastroenterol 2015;21:3157-65
25 Ansari D, Williamsson C, Tingstedt B et al. Pancreaticoduodenectomy - the transition from a low- to a high-volume center. Scand J Gastroenterol 2014;49:481-84
26 Lemmens VE, Bosscha K, van der Schelling G et al. Improving outcome for patients with pancreatic cancer through centralization. Br J Surg 2011;98:1455-62
27 Birkmeyer JD, Sun Y, Wong SL, Stukel TA. Hospital volume and late survival after cancer surgery. Ann Surg 2007;245:777-83
28 Kehlet H, Wilmore DW. Multimodal strategies to improve surgical outcome. Am J Surg 2002;183:630-41
29 Neoptolemos JP, Stocken DD, Friess H et al. A randomized trial of chemoradiotherapy and chemotherapy after resection of pancreatic cancer. N Engl J Med 2004;350:1200-10
30 Neoptolemos JP, Stocken DD, Bassi C et al. Adjuvant chemotherapy with fluorouracil plus folinic acid vs gemcitabine following pancreatic cancer resection: a randomized controlled trial. JAMA 2010;304:1073-81
31 Burris HA 3rd, Moore MJ, Andersen J et al. Improvements in survival and clinical benefit with gemcitabine as first-line therapy for patients with advanced pancreas cancer: a randomized trial. J Clin Oncol 1997;15:2403-13
32 Andersson R, Aho U, Nilsson BI et al. Gemcitabine chemoresistance in pancreatic cancer: molecular mechanisms and potential solutions. Scand J Gastroenterol 2009;44:782-86
33 Conroy T, Desseigne F, Ychou M et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med 2011;364:1817-25
34 Von Hoff DD, Ervin T, Arena FP et al. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine. N Engl J Med 2013;369:1691-1703
35 Boulay BR, Parepally M. Managing malignant biliary obstruction in pancreas cancer: choosing the appropriate strategy. World J Gastroenterol 2014;20:9345-53
36 Adams MA, Anderson MA, Myles JD et al. Self-expanding metal stents (SEMS) provide superior outcomes compared to plastic stents for pancreatic cancer patients undergoing neoadjuvant therapy. J Gastrointest Oncol 2012;3:309-13
37 Sohn TA, Yeo CJ, Cameron JL et al. Do preoperative biliary stents increase postpancreaticoduodenectomy complications? J Gastrointest Surg 2000;4:258-67; discussion 67-8
38 Jeurnink SM, Steyerberg EW, van Hooft JE et al. Surgical gastrojejunostomy or endoscopic stent placement for the palliation of malignant gastric outlet obstruction (SUSTENT study): a multicenter randomized trial. Gastrointest Endosc 2010;71:490-99
39 Koulouris AI, Banim P, Hart AR. Pain in patients with pancreatic cancer: prevalence, mechanisms, management and future developments. Dig Dis Sci 2017;62:861-70
40 Moningi S, Walker AJ, Hsu CC et al. Correlation of clinical stage and performance status with quality of life in patients seen in a pancreas multidisciplinary clinic. J Oncol Pract 2015;11:e216-21
41 Kaufman M, Singh G, Das S et al. Efficacy of endoscopic ultrasound-guided celiac plexus block and celiac plexus neurolysis for managing abdominal pain associated with chronic pancreatitis and pancreatic cancer. J Clin Gastroenterol 2010;44:127-34
42 Witvliet-van Nierop JE, Lochtenberg-Potjes CM, Wierdsma NJ et al. Assessment of nutritional status, digestion and absorption, and quality of life in patients with locally advanced pancreatic cancer. Gastroenterol Res Pract 2017;2017:6193765
43 Sikkens EC, Cahen DL, de Wit J et al. A prospective assessment of the natural course of the exocrine pancreatic function in patients with a pancreatic head tumor. J Clin Gastroenterol 2014;48:e43-6
44 Tseng DS, Molenaar IQ, Besselink MG et al. Pancreatic exocrine insufficiency in patients with pancreatic or periampullary cancer: A systematic review. Pancreas 2016;45:325-30
45 Joffe RT, Rubinow DR, Denicoff KD et al. Depression and carcinoma of the pancreas. Gen Hosp Psychiatry 1986;8:241-45
46 Holland JC, Korzun AH, Tross S et al. Comparative psychological disturbance in patients with pancreatic and gastric cancer. Am J Psychiatry 1986;143:982-86
47 Makrilia N, Indeck B, Syrigos K, Saif MW. Depression and pancreatic cancer: a poorly understood link. JOP 2009;10:69-76
48 Andersen DK, Andren-Sandberg A, Duell EJ et al. Pancreatitis-diabetes-pancreatic cancer: summary of an NIDDK-NCI workshop. Pancreas 2013;42:1227-37
49 Pannala R, Basu A, Petersen GM, Chari ST. New-onset diabetes: a potential clue to the early diagnosis of pancreatic cancer. Lancet Oncol 2009;10:88-95
50 Cui Y, Andersen DK. Pancreatogenic diabetes: special considerations for management. Pancreatology 2011;11:279-94
51 Roberts KJ, Prasad P, Steele Y et al. A reduced time to surgery within a 'fast track' pathway for periampullary malignancy is associated with an increased rate of pancreatoduodenectomy. HPB (Oxford) 2017;19:713-20
52 Jamieson NB, Chang DK, Grimmond SM, Biankin AV. Can we move towards personalised pancreatic cancer therapy? Expert Rev Gastroenterol Hepatol 2014;8:335-38
53 National Institute for Health and Care Excellence. NG12. Suspected cancer: recognition and referral. NICE. London. 2015 www.nice.org.uk/guidance/ng12
[Last accessed 29 June 2018]
54 Pancreatic Cancer Action. Pancreatic cancer symptoms & signs. https://pancreaticcanceraction.org/about-pancreatic-cancer/symptoms/[Last accessed 24 June 2018]
55 BMJ Best Practice. Pancreatic Cancer differentials. 2017 https://bestpractice.bmj.com/topics/en-gb/265/differentials. [Last accessed 30 June 2018]
56 Hartwig W, Buchler MW. Pancreatic cancer: current options for diagnosis, staging and therapeutic management. Gastrointest Tumors 2013;1:41-52