= Registered users
= Registered users = Paid-up subscribers
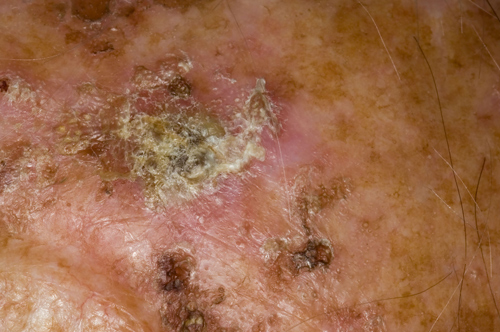
= Paid-up subscribersActinic keratoses
This condition is caused by cumulative exposure to UV light, and approximately 3-5% of lesions will transform to invasive squamous cell carcinoma. Incidence increases with age, with 40% of those over 40 having at least one lesion. Affected skin looks inflamed with a surface crust, which may be subtle. Sun-exposed skin is more commonly affected especially the head and hands in men. Management includes advice about avoiding further UV light exposure and treatment of lesions with topical preparations such as 5 fluorouracil, imiquimod, topical diclofenac 3% gel, photodynamic therapy and cryotherapy.
Asteatotic eczema
Asteatotic eczema of the lower limbs occurs secondary to dehydration, contact irritation from soaps and malnutrition. The skin has a typical cracked mosaic-like appearance. It is more common in the winter months in houses that are centrally heated with low humidity. Men are more frequently affected than women with the average age of presentation being 69. The differential diagnosis includes cellulitis, contact dermatitis, stasis eczema and thrombophlebitis. Although a biopsy is rarely required, histologically the appearance is very similar to mild sub-acute eczema. Management includes regular application of emollients, avoiding soaps and other irritants, taking short baths and avoiding high water temperatures, and the use of humidifiers. In more severe cases, topical corticosteroid ointments, with or without occlusion, can be used.
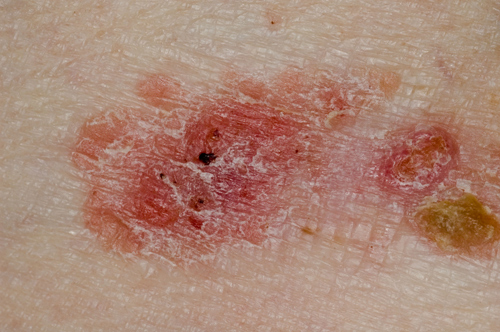
Bowen’s disease
Bowen’s disease is a squamous cell carcinoma in situ with the potential for significant lateral spread. It is seen equally frequently in men (head and neck) and women (lower limbs and cheeks) and usually occurs after the age of 60. Lesions are typically asymptomatic, red, erythematous plaques which slowly enlarge and in the early stages may only involve subtle changes which often means the diagnosis is delayed. With time 3-5% will undergo transformation to invasive squamous cell carcinoma so treatment is usually undertaken. In most cases a topical agent such as 5 fluorouracil or imiquimod can be applied. Where available photodynamic therapy can also be used or more traditional treatments such as excision, curettage or cryotherapy.
Seborrhoeic keratoses
Seborrhoeic keratoses are the most common benign tumours of the elderly. The lesions may vary in size, shape and colour and generally appear after the age of 40. They are more common on areas of skin exposed to sunlight. The cause is unknown, but an autosomal dominant mode of inheritance may be involved. Dermoscopy can be useful in differentiating between seborrhoeic keratoses and melanocytic lesions, after which reassurance can be given about the potential for malignant transformation. Treatment is not necessary but if required, for cosmetic reasons, cryotherapy or curettage and cautery can be used. Very rarely the sudden appearance of multiple eruptive seborrhoeic keratoses may indicate the Leser-Trélat sign occurring secondary to an underlying internal malignancy.
Basal cell carcinoma
The exact cause of basal cell carcinoma is unknown but environmental and genetic factors play an important part in the aetiology. Basal cell carcinoma is the most common type of skin cancer, accounting for 80% of cases. There is a doubling of incidence with every 25 years increase in age. The estimated lifetime incidence is 33-39% for men and 23-28% for women. Basal cell carcinomas rarely metastasise and as such are usually not fatal. The differential diagnosis includes sebaceous hyperplasia, Bowen’s disease, squamous cell carcinoma, actinic keratoses and Molluscum contagiosum. If in doubt, a punch biopsy from the edge of the lesion can be helpful prior to treatment. Management options include excision, photodynamic therapy, radiotherapy, cryotherapy and curettage and cautery.
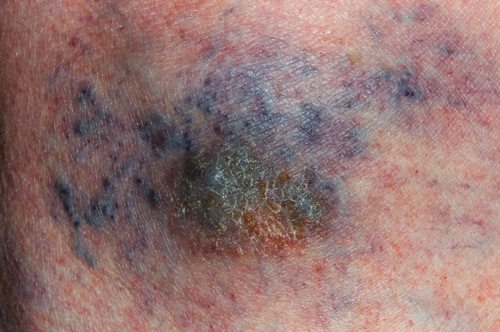
Varicose eczema
Also known as gravitational or stasis eczema this condition is common on the lower legs of older patients with varicose veins. Varicose eczema occurs as a result of increased venous pressure secondary to poor venous return and is exacerbated by the effects of gravity. Affected skin may have increased pigment secondary to the deposition of haemosiderin and in more advanced cases fibrosis and atrophic changes may occur. Treatment, as with other types of eczema, includes emollients and topical steroids along with reduction of the venous pressure by compression hosiery and elevation of affected limbs.