= Registered users
= Registered users = Paid-up subscribers
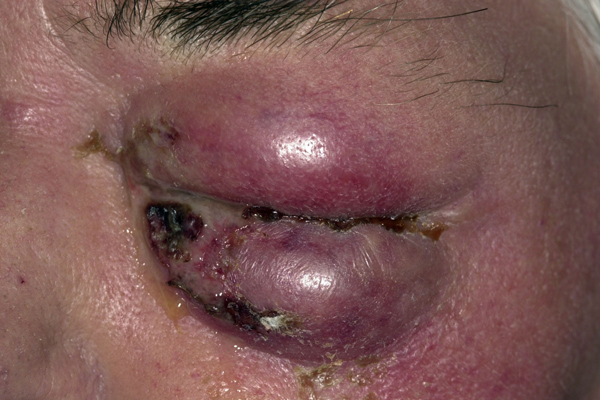
= Paid-up subscribersEczema herpeticum
Eczema herpeticum is a disseminated viral infection of the skin characterised by vesicles and punched out erosions, and associated fever. It usually occurs in patients with underlying atopic eczema who become infected with Herpes simplex type 1 or 2. It is generally associated with a first episode of Herpes simplex presenting 5 to 12 days after contact with an infected individual. It can affect any age group but is most commonly seen in infants and children. Recurrence is uncommon. The vesicles are typically monomorphic and may be purulent, or contain blood. New lesions are umbilicated, while older lesions will crust and form erosions. Regional lymphadenopathy is common and patients are usually unwell and pyrexial. In severe cases other organs may be affected including the eyes, brain, lungs and liver and the condition may be fatal. Eczema herpeticum is one of the few dermatological emergencies. Treatment consists of IV aciclovir and antibiotics for any secondary infections. Topical steroids can be used to treat any active dermatitis but are not recommended for the actual eczema herpeticum lesions.
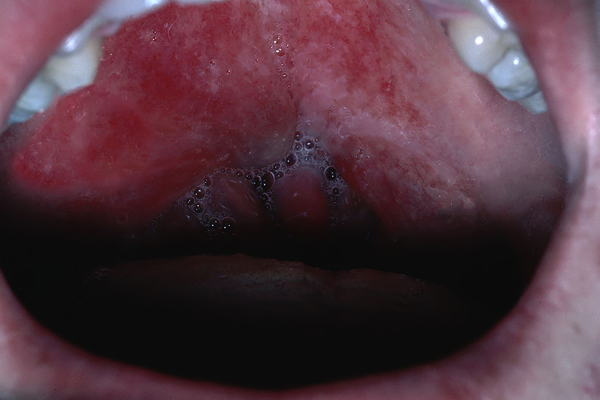
Pemphigus vulgaris
Pemphigus vulgaris is a potentially life-threatening autoimmune mucocutaneous disease with a mortality rate of 5-15%. It presents with flaccid blisters on the skin and mucous membranes, which may be associated with localised erythema. The affected areas are usually painful but rarely pruritic and are fragile, breaking open to leave painful erosions. The cause of the condition remains unknown but several potentially relevant factors include genetic predisposition, older age and an association with other autoimmune conditions such as myasthenia gravis and thymoma. Treatment consists of oral steroids and immunosuppressive drugs.
Perinephric abscess
An abscess is a collection of suppurative material anywhere in the body. In this case the abscess was in the perinephric space around the left kidney. Diagnosing perinephric abscesses can be a challenge as the symptoms are often very non-specific. This patient presented with a low-grade fever, pain in the left flank, lethargy, weight loss and then a mild erythema over the area of pain. The diagnosis was confirmed by a CT scan and she was treated with a drain, to remove the pus, and IV antibiotics.
Quinsy
Quinsy, or peritonsillar abscess, is usually a complication of acute exudative tonsillitis, but may occur alone. Pus collects between the tonsillar capsule and lateral pharyngeal wall causing symptoms which may include severe pain, difficulty swallowing, fever, distortion of vowels on speaking, the so-called ‘hot potato voice' and drooling of saliva. Unlike tonsillitis, which is usually treated with oral antibiotics, quinsy may require admission for IV antibiotics and rehydration with incision and drainage of the abscess. Untreated complications can include necrotising fasciitis, and in severe cases airway obstruction.
Necrotising fasciitis
First described in 1848, necrotising fasciitis is a severe form of infection which spreads rapidly through soft tissue and is often fatal. The common causative organisms are group A beta-haemolytic streptococci, although in some cases a combination of organisms may be responsible for the infection. Necrotising fasciitis may arise as a complication of procedures such as cardiac catheterisation, vein sclerotherapy, diagnostic laparoscopy or certain medical conditions such as quinsy or any condition that causes immunodeficiency or requires oral steroids. It develops very quickly and once diagnosed needs urgent treatment. This includes antibiotics, hyperbaric oxygen, and surgical debridement of all affected tissue. Both sepsis and renal failure are potential complications and the mortality rate is around 25%.