SEARCH
 = Registered users
= Registered users = Paid-up subscribers
= Paid-up subscribersEpee-Bekima M, Overton C. Diagnosis and treatment of ectopic pregnancy. Practitioner 2013;257 (1759):15-17
Diagnosis and treatment of ectopic pregnancy
21 Mar 2013
AUTHORS
Mr Mathias Epee-Bekim MD MRCOG, Senior Registrar in Obstetrics and Gynaecology
Mrs Caroline Overton MBBS MD FRCOG FHEA, Consultant in Obstetrics and Gynaecology, Subspecialist in Reproductive Medicine & Laparoscopic Surgery
St Michael’s Hospital, Bristol, UK
Article
An ectopic pregnancy occurs when a fertilised egg is implanted outside the uterus. The most common site is the fallopian tube; rarely an ectopic pregnancy can be found in the ovary, a caesarean section scar, the abdomen or the cervix.
The most common risk factors are:
• Previous ectopic pregnancy
• Pelvic inflammatory disease
• Endometriosis
• Previous pelvic surgery
• Presence of a coil
• Infertility
However, a third of women with an ectopic pregnancy have no known risk factors.
Ectopic pregnancy occurs in an average of 1 in 90 pregnancies in the UK. Although most cases are recognised and treated appropriately, women still die as a result of late diagnosis and suboptimal management of ectopic pregnancy. Six women died as a result of ectopic pregnancy between 2006 and 2008 in the UK.1 The NICE guideline on ectopic pregnancy and miscarriage, published in December 2012, recommends a low threshold for offering a pregnancy test to womenof childbearing age when they attend the surgery.2
Women should be referred to the most appropriate unit (A&E, gynaecology or early pregnancy assessment (EPA) service) if an ectopic pregnancy is suspected. The guideline also emphasises the need to give practical support and information to patients and their partners.
Signs and symptoms
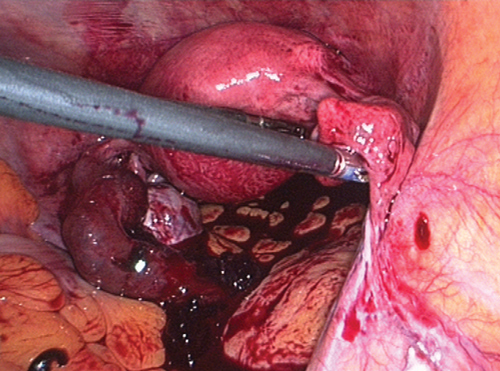
In early pregnancy, all ectopic pregnancies will be asymptomatic; symptoms and signs appear when the tube starts to tear, see table 1. When the tube ruptures, the woman will quickly become unwell and haemodynamically unstable because of rapid intra-abdominal blood loss, see figure 1.
Because of the range of symptoms a pregnancy test should be offered to all women of reproductive age.
It is important to remember that a positive diagnosis of a urinary tract infection or gastroenteritis does not exclude an ectopic pregnancy.
Examination and assessment
A basic examination should include general appearance (to look for pallor, shock, collapse), pulse (for tachycardia > 100 beats/minute) blood pressure (hypotension i.e. < 100/60 mmHg) and orthostatic hypotension.
The signs to look for in a case of suspected ectopic pregnancy are shown in table 2.
Referral
The urgency and location of the referral depends on the clinical situation.
Women who are haemodynamically unstable, or in whom there is significant concern about the degree of pain or bleeding, should be referred directly to A&E, irrespective of the result of the pregnancy test. Women may sometimes be unable to pass urine if they are hypovolaemic.
Stable patients with bleeding who have pain or a pregnancy of six weeks gestation or more or a pregnancy of uncertain gestation should be referred immediately to an EPA service (or out-of-hours gynaecology service if the EPA service is not available) for further assessment. There are more than 200 NHS EPA units throughout the UK with different working hours (see External websites).
If the EPA service is closed and you are concerned about the patient, contact the gynaecologist on call, with a view to avoiding delay in further assessment. It is important to explain to the patient, and her partner, why she is being referred and what to expect when they arrive at the hospital.
GPs can use expectant management for women with a pregnancy of less than six weeks gestation who are bleeding but who are not in pain. They should advise these women to repeat a urine pregnancy test after 7–10 days and to return if it is positive or if their symptoms continue or worsen. The patient and her partner should be given a phone number to call in an emergency. The development of pain should prompt referral. An EPA service or out-of-hours gynaecology service should be contacted immediately when pain develops. If the pain is severe, the patient should be referred to A&E.
Confirming diagnosis
After a positive pregnancy test at the surgery, the diagnosis will be confirmed, at the EPA service or out-of-hours gynaecology service, via a transvaginal ultrasound scan to identify the location of the pregnancy.
If a transvaginal ultrasound scan is unacceptable to the woman, she will be offered a transabdominal ultrasound scan, which has visual limitations but has the advantage of being able to detect fibroids, an enlarged uterus and ovarian cysts.
If the ultrasound is inconclusive and the pregnancy cannot be located, human chorionic gonadotrophin (hCG) levels repeated after 48 hours may help to make a diagnosis and assist in planning the repeat scan.
hCG is an indicator of trophoblast proliferation but not the location of the pregnancy. It should be noted that hCG can increase, decrease or plateau with an ectopic pregnancy. The ultrasound scan and the woman’s symptoms are the key to diagnosis.
If the diagnosis is still unclear and the woman is in significant pain, a laparoscopy may be offered.
Management
The management options depend on the symptoms, the hCG level, the ultrasound findings, the patient’s general health and preferences, and the facilities for follow-up.
Medical management
Medical management with methotrexate is offered to women who are able to return for follow-up and who fulfill all the following criteria:
• No significant pain
• An unruptured ectopic pregnancy with an adnexal mass smaller than 35 mm with no visible heartbeat
• A serum hCG < 1,500 IU/L
• No intrauterine pregnancy (as confirmed on an ultrasound scan).
Methotrexate is an antimetabolite and antifolate drug. It is teratogenic and effective contraception should be used for three months following administration. Patients should avoid alcohol and NSAIDs. Approximately one in six women will experience side effects of nausea, sickness, diarrhoea, mouth ulcers and feelings of fatigue. These symptoms usually only last a few days.
Monitoring is hospital based. Women are asked to attend regularly for blood tests (including liver and renal function) and hCG follow-up until levels are < 25 IU/L. A Rhesus-negative woman will not need to receive anti D.
An ectopic pregnancy may rupture despite apparently successful treatment and declining hCG levels. Significant pain during medical treatment with methotrexate would indicate a ruptured ectopic pregnancy and should prompt emergency assessment and hospital admission.
Surgery
Surgical management usually laparoscopic salpingectomy (unless there is an abnormal contralateral tube or the patient is haemodynamically unstable), will be offered to women who are unable to return for follow-up after methotrexate treatment or who have an ectopic pregnancy plus any of the following:
• Significant pain
• An adnexal mass of 35 mm or larger
• A fetal heartbeat visible on an ultrasound scan
• A serum hCG > 5,000 IU/L
Rhesus-negative women undergoing surgery for ectopic pregnancy should be offered 250 IU anti D.
Expectant management
This is outside the remit of the NICE guidance, but could be considered for a pain-free woman with a small ectopic pregnancy, able to return for follow-up, with low and falling hCG levels. The protocols vary at each hospital. A third of these women will require additional medical or surgical management.
Conclusion
NICE recommends pregnancy testing of women of reproductive age presenting with both common and less common symptoms and signs of ectopic pregnancy and a low threshold for referral to the EPA, out-of-hours gynaecology service or A&E. There is a strong emphasis on communication and support throughout the whole process.
NICE has made a priority recommendation that EPA services should be available seven days a week facilitating access to ultrasound scanning. Women who have had a previous ectopic pregnancy may self-refer to an EPA service.
The guidance also promotes medical management of ectopic pregnancy for suitable patients and laparoscopy (rather than laparotomy) for women who require surgery.
REFERENCES
1 Centre for Maternal and Child Enquiries (CMACE). Saving Mothers’ Lives: reviewing maternal deaths to make motherhood safer: 2006–08. The Eighth Report on Confidential Enquiries into Maternal Deaths in the United Kingdom. BJOG 2011;118 (Suppl. 1):1–203
2 National Institute for Health and Clinical Excellence. CG154. Ectopic pregnancy and miscarriage: diagnosis and initial management in early pregnancy of ectopic pregnancy and miscarriage. NICE. London. 2012
3 Royal College of Obstetricians and Gynaecologists. The management of tubal pregnancy. RCOG Guideline No 21. RCOG. London. 2010
ARTICLE IN PDF
PRESET SEARCHES
PubMed
Ectopic pregnancy - reviews
NICE Evidence Search
Immediate CPD prompts
These handy templates* prompt immediate drafting of personal learning, reflection and planning. Save your record straight into your personal development folder on your device or Cloud storage system.
*Adobe reader needed for iPad
EXTERNAL WEBLINKS
Early Pregnancy Assessment Units
To find your local EPA unit go to http://earlypregnancy.org.uk/FindUsMap.asp
NHS choices
www.nhs.uk/conditions/Ectopic-pregnancy
The Ectopic Pregnancy Trust