SEARCH
 = Registered users
= Registered users = Paid-up subscribers
= Paid-up subscribersCPD frameworks
These frameworks, associated with all articles, prompt drafting of personal learning, reflection and planning.
Save your reflective note into your device or cloud
Fillable PDF frameworks
Adobe reader needed for tablets
Word frameworks - for reflective practice
Click to download
Reflection on a journal article
Stages of reflection on a situation
Reflection of a team, practice or group
External reference on reflection
Reflective practice in health care and how to reflect effectively
Koshy K, Limb C et al. International Journal of Surgical Oncology. 2017 2:e20
Griffiths C, Levy ML. Preventing avoidable asthma deaths. Practitioner 2014; 258 (1774)27-31
Preventing avoidable asthma deaths
23 Sep 2014
AUTHORS
Professor Chris Griffiths FRCP FRCGP, Asthma UK Centre for Applied Research, Centre for Primary Care and Public Health, Blizard Institute, London, UK
Dr Mark L Levy FRCGP, Part-time sessional GP and Clinical Lead National Review of Asthma Deaths (NRAD) - 2011-2014
Article
Abstract
The UK has one of the highest death rates in Europe from asthma, with more than 20 people dying from the disease each week. Across the UK there is a five-fold variation in the number of hospital admissions for asthma almost certainly explained in part by variations in delivery, uptake and organisation of care. Deaths from asthma are frequently avoidable the findings from the National Review of Asthma Deaths have confirmed. A total of 276 cases were considered by the confidential enquiry panels and 195 confirmed as asthma deaths. Major avoidable factors were judged to be present in 60% of cases. Key findings from the report include: Almost half the patients (45%) died without seeking medical help or before help could be provided; 10% died within 28 days of discharge from hospital; 21% had attended A&E with asthma in the previous year; and only 23% had a personal asthma action plan. Over-prescription of short-acting bronchodilators and under-prescription of preventer inhalers was common. Every general practice should have a designated, named clinical lead for asthma services. Patients with asthma should be referred to a specialist asthma service if they have required more than two courses of systemic corticosteroids, oral or injected, in the previous 12 months or management using BTS steps 4 or 5 to achieve control. Any patient admitted to hospital or attending A&E with asthma should be reviewed, and control optimised, within a week of discharge. All asthma patients should have a written personal asthma action plan and should have a structured review by a healthcare professional with training in asthma at least annually.
Deaths from asthma are frequently avoidable the findings from the national Review of Asthma Deaths (NRAD), published in May this year on World Asthma Day, have confirmed.1
The UK has one of the highest death rates in Europe from asthma,2 with more than 20 people dying from the disease each week. Over the past 50 years, death rates initially fell, but in the past 20 years this trend has faltered.3
Asthma deaths can be seen as the tip of an iceberg. For each death there are many patients who have narrowly avoided death, who have been admitted to hospital for asthma, attended A&E departments or have presented as an emergency in general practice.
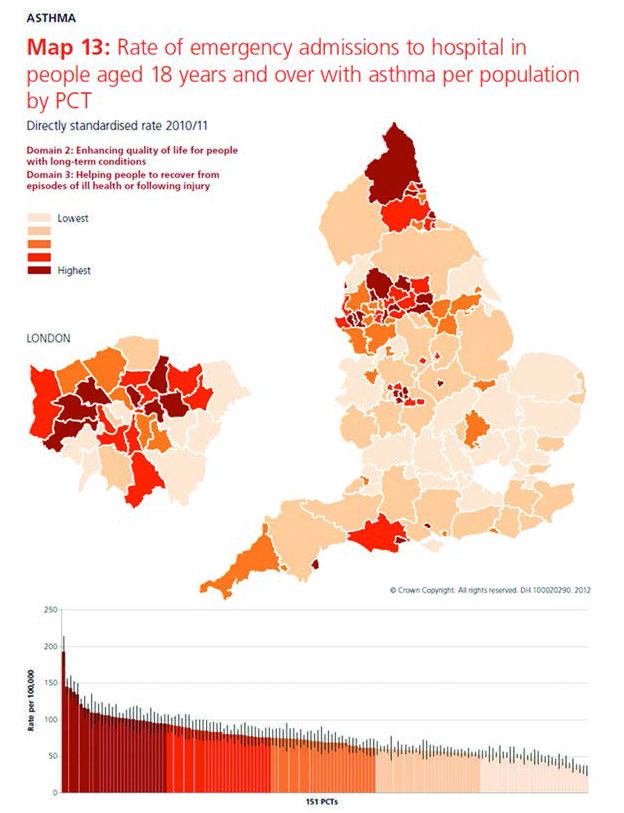
Across the UK there is a five-fold variation in the number of hospital admissions for asthma, almost certainly explained in part by variations in delivery, uptake and organisation of care, see figure 1.4
The NRAD has important implications for asthma care generally, as well as preventing deaths.
Methodology
Confidential enquiries use case-based review, whereas evidence-based guidelines use systematic review of the published literature,5 and so have the potential to generate different insights. The two can be seen as complementing each other.
There have been previous reviews of asthma deaths,6-12 each highlighting potentially avoidable causes, see table 1. With no sign of further reductions in deaths from asthma this review was set up to provide the most up-to-date and comprehensive assessment of causes and possible remedies.
The NRAD is the first UK-wide review of asthma deaths, prospectively collecting details on deaths in hospital and in the community. Other new features are the inclusion of reports from out of hours services, paramedics, coroners and ambulance services, as well as weather and air quality data.
The NRAD was run by a consortium of asthma professional and patient bodies, led by the Royal College of Physicians, London. It examined the circumstances surrounding deaths from asthma over a one-year period, starting in February 2012. Deaths were reviewed systematically and were subject to an in-depth multidisciplinary confidential enquiry.
Between February 2012 and January 2013, all asthma deaths in the UK were identified through the Office for National Statistics (ONS) for England and Wales, the Northern Ireland Statistics and Research Agency (NISRA) and the National Records of Scotland (NRS).
Details about 900 selected deaths were collected from various sources including primary, secondary and tertiary care, as well as ambulance, paramedic and out-of-hours care providers.
A total of 374 local co-ordinators were appointed in 297 hospitals to collect information, and 174 clinical assessors were recruited to expert panels that reviewed data.
Each assessor took part in one or more expert panels during which all information gathered on each death was reviewed by two assessors in detail. This was followed by discussion and a consensus agreement of avoidable factors and recommendations by the whole panel.
Cases reviewed at the confidential enquiry panels were those where the notifying clinicians were confident either on notification or subsequent discussion with the NRAD project team that asthma was the cause of death, or those cases considered difficult to define by notifying clinicians.
Panellists included: consultants in respiratory medicine, paediatrics, emergency medicine or paediatric emergency medicine, intensive care or paediatric intensive care; GPs; respiratory nurse specialists in primary, acute and secondary care; and pharmacists.
Key findings
A total of 276 cases were considered and 195 confirmed as asthma deaths. The median age at death was 58 years, range 4-97. The median age at diagnosis was 37 years (range 10 months-90 years), with a median duration of asthma of 11 years (range 0-62 years).
Major avoidable factors were judged to be present in 60% of cases.
Some of the most striking findings from the report were that:
• Almost half the patients (45%) died without seeking medical help or before help could be provided
• One in ten patients (10%) died within 28 days of discharge from hospital
• One in five (21%) had attended A&E with asthma in the previous year
• Fewer than one in four (23%) had a personal asthma action plan (PAAP)
• Over-prescription of short-acting bronchodilators and under-prescription of preventer inhalers was common.
Full lists of key findings from the report are summarised in boxes 1 to 4.
The following case study illustrates some of the typical features of asthma deaths the panels encountered. This is a composite, drawn from a number of cases, to generate anonymity and to illustrate a theme.
Case study
Stephen was a 47-year-old man whose asthma had been diagnosed at the age of 12. His GP classified his asthma as mild – his repeat prescription list consisted of salbutamol and a low-dose beclometasone metered dose inhaler.
He died at his home in the early hours of a Sunday morning, before the ambulance arrived.
When the expert panel assessed his records they found that his last asthma review had occurred two years before his death. His records from his last review suggested he had asthma symptoms on most days. He used his salbutamol inhaler at least two or three times on most days.
His latest peak expiratory flow rate was 120 L/min, with a previous best of 260 L/min and a predicted value of 426 L/min.
At his last review his GP had added a beclometasone inhaler to his treatment. He did not attend a follow-up appointment, but was seen twice for unrelated symptoms over the next two months.
He had visited A&E with an asthma attack eight months before his death. He had seen his GP four months before death with breathlessness and wheeziness, when he had been prescribed an antibiotic only. He had been seen three times subsequently for arthritis symptoms.
His prescribing record showed that he had been issued prescriptions for 18 salbutamol inhalers and one beclometasone 100 mcg (200 doses) inhaler in the previous year.
Avoidable factors in this case include: failure to attend for asthma reviews – notably following an A&E attendance; poor asthma control reflected in a prescribing pattern of an excess of salbutamol inhalers and only one preventer inhaler, and a low peak expiratory flow rate.
Putting in place systems that ensure people are reviewed within days of an A&E attendance, and flag up failure to attend a review, excess salbutamol prescribing and poor control could have prevented this man’s death. Exactly what these systems are and how they work may require a combination of centrally developed systems e.g. by computer suppliers, and changes in the way general practices organise care. However, they largely consist not of major innovations, but of improvements in the organisation of routine care, already emphasised in national guidelines.5
Implications for primary care
The report’s goal is not to apportion blame but to highlight learning opportunities to change practice and thereby reduce deaths.
It makes extensive recommendations for improving services in both primary and secondary care.
The first response for primary care teams should be to nominate a clinician trained in asthma care as having overall responsibility for asthma. This lead clinician should ensure the team meets to take a fresh view of asthma care in the practice.
Asthma review and optimising control
It is important to ensure that any patient admitted to hospital or attending A&E with asthma is reviewed, and control is optimised, within a week of discharge.
Screening discharge letters and developing a system that not only triggers invitations but also monitors attendance is needed.
Consider introducing simple questionnaires that score asthma control such as the asthma control test.
Both doctors and nurses should be up to date with asthma training. Ensure nurses are empowered to refer people with poor control for immediate or urgent reviews with doctors.
Rescue medication and action plans
Patients who have had severe asthma attacks should have rescue courses
of prednisolone at home with clear instructions on self-initiation.
Self-management plans improve asthma control and prevent attacks.
All patients should have a written plan.
Patients need to know how and when to seek care. Practices, including receptionist teams, need to ensure any patient calling with poor asthma control can be seen on the same day.
Adequate treatment and follow-up
Asthma attacks are frequently undertreated, either with antibiotics or advice to increase inhaler use. Oral prednisolone is one of the most effective treatments for acute severe asthma and should be used more frequently.
Any patient attending the practice with an attack should be followed up within a week. Asthma attacks are an ideal opportunity to educate patients, identify triggers and plan for future avoidance and actions.
Systems to identify and address inappropriate prescribing should be developed. Any patient needing one short-acting beta-agonist inhaler or more per month needs a review of their control, adherence and use of preventer medication.
Risk factors
Psychosocial problems, learning disabilities and obesity were present alone or in combination in around 50% of deaths. These risk factors should alert teams for the need for extra vigilance.
The NRAD recommends referring any patient with two or more courses of prednisolone within the past year, or treated at step 4 or 5 of the British Thoracic Society (BTS) guidelines.
Key recommendations to improve care
Organisation of NHS services
All hospitals and general practices should have a named clinical lead for asthma services, with responsibility for training in the management of acute asthma.
Patients should be referred to a specialist service if they have needed more than two courses of systemic corticosteroids, oral or injected, in the past year or management using BTS steps 4 or 5.1
Follow-up arrangements should be made after every attendance for an asthma attack at an A&E department or out-of-hours service.
Secondary care follow-up should be arranged after every admission for asthma, and for those who have attended A&E two or more times with an asthma attack in the past year.
There is an urgent need for electronic surveillance of prescribing in primary care to alert clinicians to inappropriate prescribing.
The report recommends the development of a standard national asthma template to facilitate a structured, thorough asthma review. This should improve the documentation of reviews in medical records and form the basis of local audit of asthma care.
A national ongoing audit of asthma deaths should also be established.
Medical and professional care
All asthma patients should have a written PAAP. At least once a year, they should have a structured review by a healthcare professional with specialist training in asthma.
Factors that trigger or exacerbate asthma should be elicited and documented in medical records and PAAPs of all patients with asthma.
Asthma control should be assessed at every asthma review. Where loss of control is identified, immediate action is essential including optimisation of treatment, possible referral to a colleague with greater asthma expertise, and arrangements for follow-up and review.
Healthcare professionals must be aware of factors that raise the risk of asthma attacks and death, including concurrent psychological and mental health problems.
Prescribing and medicines use
All patients who have been prescribed more than 12 short-acting reliever inhalers in the past year should be invited for urgent review.
An assessment of inhaler technique should be routinely undertaken and formally documented at annual review. This should be checked by the pharmacist when a new device is dispensed.
Non-adherence with preventer inhaled corticosteroids should be continually monitored as it is associated with increased risk of poor asthma control.
The use of combination inhalers should be encouraged. A long-acting beta-agonist should be prescribed with an inhaled corticosteroid in a single combination inhaler.
Patient factors and perception of risk
Self-management should be encouraged with respect to triggers e.g. increasing medication before the start of the hay fever season, avoiding NSAIDs, or early use of oral corticosteroids with viral or allergic-induced exacerbations.
A history of smoking and/or exposure to second-hand smoke should be noted in patients’ records. Smokers should be offered referral to a smoking cessation service.
Parents, carers, teachers and children should be educated about managing asthma. This should cover how, why and when to use asthma medications, recognising when asthma is not controlled and knowing when and how to seek emergency advice.
Minimising exposure to allergens and second-hand smoke is important especially in young people with asthma.
Conclusion
The NRAD is the largest and most comprehensive review to date of the circumstances surrounding asthma deaths. It has proposed a series of changes to improve asthma care.
Some of these are new and others have been highlighted by previous confidential enquiries, but most can be readily implemented by clinical teams with better organisation and without major changes in staffing or workload. Every death from asthma is a tragedy, but most are avoidable.
Acknowledgement
This report was commissioned by the Healthcare Quality Improvement Partnership (HQIP) on behalf of NHS England, NHS Wales, the Health and Social Care Division of the Scottish Government, and the Northern Ireland Department of Health, Social Services and Public Safety (DHSSPS). The report was delivered by the Clinical Effectiveness and Evaluation Unit (CEEU) of the Clinical Standards Department at the Royal College of Physicians (RCP).
REFERENCES
1 Royal College of Physicians. Why asthma still kills: the National Review of Asthma Deaths (NRAD) Confidential Enquiry report. RCP. London. 2014 www.rcplondon.ac.uk/sites/default/files/why-asthma-still-kills-full-report.pdf
2 Wolfe I, Cass H, Thompson MJ et al. Improving child health services in the UK: insights from Europe and their implications for the NHS reforms. BMJ 2011 Mar 8;342:d1277. doi: 10.1136/bmj.d1277
3 Department of Health. An Outcomes Strategy for Chronic Obstructive Pulmonary Disease (COPD) and Asthma in England. DH. London. 2011
4 www.rightcare.nhs.uk/index.php/atlas/respiratorydisease
5 British Thoracic Society/Scottish Intercollegiate Guidelines Network. British Guideline on the Management of Asthma (Updated online 2013). Thorax 2008;63 (Supplement 4): iv1- iv121 www.sign.ac.uk/ guidelines/fulltext/101/index.html
6 MacDonald JB, MacDonald ET, Seaton A, Williams DA. Asthma deaths in Cardiff 1963-74: 53 deaths in hospital. Br Med J 1976;2:721-23
7 MacDonald JB, Seaton A, Williams DA. Asthma deaths in Cardiff 1963-74: 90 deaths outside hospital. Br Med J 1976;1:1493-95
8 Ormerod LP, Stableforth DE. Asthma mortality in Birmingham 1975-7: 53 deaths. Br Med J 1980;280:687-90
9 Masters N. Death from asthma in two regions of England. Br Med J 1982;285:1570-71
10 Ross Anderson H, Ayres JG, Sturdy PM. Bronchodilator treatment and deaths from asthma: case-control study. Br Med J 2005;330:117-23
11 Wareham NJ, Harrison BD, Jenkins PF et al. A district confidential enquiry into deaths due to asthma. Thorax 1993;48(11):1117-20
13 www.asthma.org.uk/Sites/healthcare-professionals/pages/self-management-materials