SEARCH
 = Registered users
= Registered users = Paid-up subscribers
= Paid-up subscribersCPD frameworks
These frameworks, associated with all articles, prompt drafting of personal learning, reflection and planning.
Save your reflective note into your device or cloud
Fillable PDF frameworks
Adobe reader needed for tablets
Word frameworks - for reflective practice
Click to download
Reflection on a journal article
Stages of reflection on a situation
Reflection of a team, practice or group
External reference on reflection
Reflective practice in health care and how to reflect effectively
Koshy K, Limb C et al. International Journal of Surgical Oncology. 2017 2:e20
Stollery N. Photoguide:Skin conditions in children. Practitioner 2016;260(1789):28-29
Skin conditions in children
25 Jan 2016
AUTHORS
Dr Nigel Stollery MB BS DPD, GPwSI Dermatology, Kibworth, Leicestershire, UK
Article
Classic spitz naevus
Spitz naevus is a rare type of rapidly growing benign naevus that affects children. In 70% of cases naevi are found on the limbs or face. Once fully formed they may remain unchanged for a number of years after which spontaneous regression can occur. They are typically dome shaped and there are two types, the classic red and the pigmented brown type. Spitz naevi can be up to 2 cm in diameter and may be difficult to distinguish from malignant melanomas. Although treatment is not usually necessary, where there is true diagnostic doubt excision is recommended.
Irritant saliva dermatitis
In this form of contact dermatitis the skin is damaged by persistent contact with saliva. The degree of damage depends on the amount of contact, the frequency of exposure, skin susceptibility and environmental factors such as heat and humidity. The most commonly affected areas in children are the lips, from repeated licking, but in this case the child had a habit of sucking his index finger. No other areas of his body were affected. Management involves avoiding contact of affected areas with saliva and very regular application of a greasy emollient which acts as a barrier. If there is secondary infection or marked inflammation then topical antibiotics and steroids can be helpful.
Umbilical granuloma
Umbilical granuloma is a relatively common condition that occurs during the umbilical healing phase following separation of the umbilicus in the postnatal period. The granuloma is typically a small pink painless swelling containing fibroblasts and capillaries, which usually looks moist and may discharge a clear or yellow fluid. Allowing the granuloma to be exposed to air by rolling the nappy down can help to dry the area and promote healing. If healing is slow the application of table salt, directly onto the area for 10-30 minutes under a gauze, twice daily for five to seven days can help. In more persistent cases the application of silver nitrate will help reduce the granulation tissue and promote healing. In cases which do not respond to silver nitrate differential diagnoses to consider are umbilical polyps and granulomas secondary to a patent urachus.
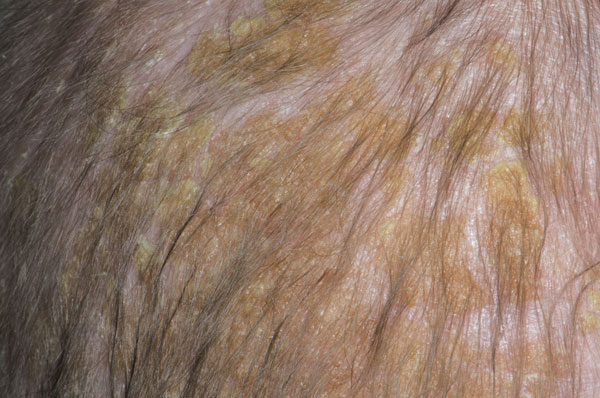
Cradle cap
Neonatal seborrhoeic dermatitis, also known as cradle cap, is a very common condition which affects around 50% of babies. It usually develops in the first three months of life and may persist for longer than 12 months. It appears as thick, patchy, greasy, yellow scales over the scalp. It is not itchy and usually does not bother the baby at all. The cause is not clearly understood but it may be related to overactivity of the sebaceous glands in newborns caused by circulating maternal hormones. Treatment options include the application of baby oil and shampoos. In more severe cases topical antifungal preparations or hydrocortisone cream may help.
Molluscum contagiosum
Four subtypes of mollusca have been identified. The vast majority (96%) of lesions are caused by type 1. However, in patients with HIV type 2 infections are more common. Characteristic lesions are rounded dome-shaped papules 2-5 mm in size with an umbilicated centre and caseous plug. Rarely very large lesions can be seen up to 1.5 cm in diameter. In 10% of cases a perilesional eczema is seen which resolves completely once the molluscum disappears. Spread occurs by scratching, and the lesions then spread to adjacent body surfaces, or via direct skin contact between children. Treatment is not usually required in immunocompetent individuals and the condition usually spontaneously regresses two months to two years after onset.
Juvenile plantar dermatosis
This is a condition most commonly seen on the feet of boys aged between four and eight. Affected areas are dry and may have a glazed or shiny appearance. The toe webs tend to be spared unlike tinea infection where they are commonly affected. The condition arises where there is dampness and friction associated with wearing synthetic footwear and sweat-laden socks. Differential diagnoses include tinea, contact dermatitis and atopic dermatitis, keratolysis exfoliativa and psoriasis. Management involves avoiding synthetic footwear where possible, and keeping the feet dry with regular changes of cotton socks. Topical steroids are often prescribed but are rarely more effective than simple emollients which should be applied regularly.