SEARCH
 = Registered users
= Registered users = Paid-up subscribers
= Paid-up subscribersCPD frameworks
These frameworks, associated with all articles, prompt drafting of personal learning, reflection and planning.
Save your reflective note into your device or cloud
Fillable PDF frameworks
Adobe reader needed for tablets
Word frameworks - for reflective practice
Click to download
Reflection on a journal article
Stages of reflection on a situation
Reflection of a team, practice or group
External reference on reflection
Reflective practice in health care and how to reflect effectively
Koshy K, Limb C et al. International Journal of Surgical Oncology. 2017 2:e20
Stollery N. Photoguide:Pruritus. Practitioner 2015;259(1780):28-29
Pruritus
23 Mar 2015
AUTHORS
Dr Nigel StolleryMB BS DPD, GPwSI Dermatology, Kibworth, Leicestershire, UK
Article
Cholestatic pruritus
Cholestatic pruritus is associated with liver disease such as primary biliary cirrhosis, hepatitis C infection, bile duct carcinoma and primary sclerosing cholangitis. The deposition of bile salts in the skin is thought to be the cause of the widespread intense pruritus, but there is little correlation between the intensity of the itch and the degree of jaundice. In patients with complete hepatic failure the pruritus tends not to be present suggesting products made by the liver are the cause. Bile salt chelating agents have been found to be effective in reducing pruritus, but the response may be temporary. The SSRI sertraline has also been found to be effective in some patients and clinical trials are ongoing.
Phytodermatitis
Phytodermatitis is triggered by contact with plants. In this case the culprit was ivy which is a common cause of the condition. Unlike other types of dermatitis the rash may have a characteristic linear or streaky appearance. Blistering is common and the rash may be exacerbated by ultraviolet light. Postinflammatory hyperpigmentation is common which may take many months to fade. As the condition is self-limiting symptomatic treatment is usually all that is required. Topical steroids, ice packs and cold showers can improve the pruritus, but are less effective for the blistering. It is important to try to avoid all further contact with the plant, and contact with soaps and other irritants while the rash is present.
Insect bites
Insect bites are a common cause of localised pruritus. Usually the diagnosis is obvious especially if the patient has seen the insect. In other cases the rash may develop after the insect has left. The presence of localised clusters of itchy, burning papules, with circumferential erythema and swelling can be a helpful sign. Rarely more severe reactions can occur including anaphylaxis which at worst may be fatal. Where severe reactions have occurred adrenaline should be carried and administered as soon as possible after a bite. In less severe reactions antihistamines, cold compresses and simple analgesia is all that is required. In bee stings where the sting is still visible in the skin it should be scraped out as soon as possible.
Chickenpox
Chickenpox is a common childhood illness and occurs most frequently in the first decade of life. It is caused by the varicella zoster virus and approximately 90% of adults have immunity to the virus. The patient will be infectious from two days before the onset of the rash, which consists of very pruritic widespread vesicles, for around eight days. Symptomatic treatment is usually all that is required. In adults the condition may be more severe and antivirals may be prescribed. Pregnant women, newborn babies and patients who are immunosuppressed are at increased risk of more serious complications. In the UK, vaccination is currently only offered to those at increased risk.
Urticaria
Urticaria is a common cause of pruritus affecting 20% of people at some point during their lifetime. The rash, which consists of wheals, typically lasts less than 24 hours after which the skin will return to normal, but may recur. In most cases an underlying cause is not found, but viruses and certain drugs may act as triggers. The rash and pruritus is caused by the release of histamine, bradykinin, leukotriene C4, prostaglandin D2 and other vasoactive agents in the dermis. Differential diagnoses include mastocytosis, urticarial vasculitis, erythema multiforme and drug eruptions. Basic treatment includes H1 and H2 antihistamines which may be required in higher than licensed doses. In more severe cases a short course of oral steroids may be required, but this should not be repeated as rebound worsening may occur. In persistent cases referral to secondary care would be appropriate.
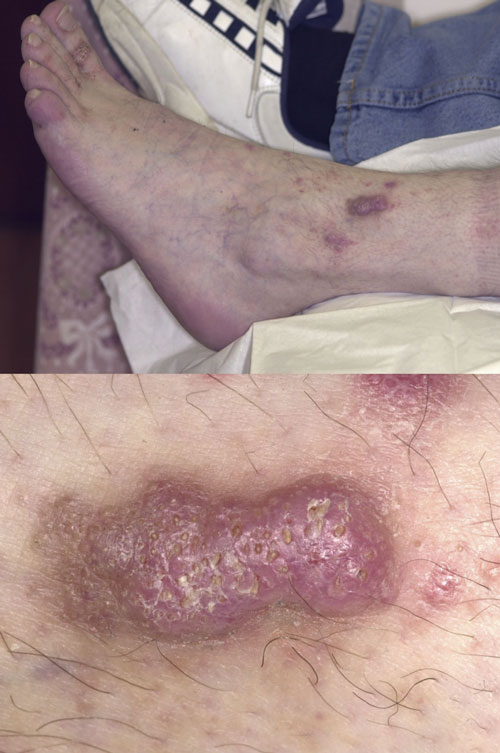
Hypertrophic lichen planus
Lichen planus is an uncommon skin condition which produces very pruritic skin lesions. The various forms include oral, classical, genital and actinic lichen planus. The nails and hair follicles can also be affected. Lichen planus is thought to result from an abnormal immune reaction to a viral infection or drug, causing inflammatory cells to attack skin cells. Around 85% of cases will clear spontaneously by 18 months and treatment is not always necessary. Where the mouth or genitals are affected the condition may be more persistent. If the diagnosis is in doubt a biopsy can be performed. Treatment options include potent topical steroids and topical immunosuppressants. In more severe cases, oral treatment with systemic steroids, methotrexate, acitretin, and hydroxychloroquine can be helpful.