SEARCH
 = Registered users
= Registered users = Paid-up subscribers
= Paid-up subscribersKirby R. The role of PSA in detection and management of prostate cancer. Practitioner 2016; 260(1792):17-21
The role of PSA in detection and management of prostate cancer
25 Apr 2016
AUTHORS
Professor Roger Kirby MA MD FRCS (Urol) FEBU, Professor of Urology, Medical Director, The Prostate Centre, London, UK
Article
Abstract
The prostate specific antigen (PSA) test clearly provides the opportunity for clinically relevant prostate cancer to be detected at a stage when treatment options are greater and outcomes may be improved. However, in some patients the PSA test may lead to investigations which can identify clinically insignificant cancers which would not have become evident in a man’s lifetime. In addition, a raised PSA may often indicate benign prostatic enlargement, and this may provide an opportunity for treatment of this condition before complications develop. The lack of sensitivity and specificity that characterises PSA testing in the initial diagnosis of prostate cancer largely disappears after treatment of localised prostate cancer, especially after surgery. Three monthly PSA measurement is usually recommended for the first year after primary treatment. Subsequently less frequent testing is required. A PSA rise after primary treatment usually indicates biochemical recurrence and often the need for further therapy. There are two promising urinary RNA biomarkers, prostate cancer antigen 3 (PCA3) and fusion gene TMPRSS2:ERG, both of which aim to distinguish between men with low-risk (indolent) and those with aggressive (clinically significant) cancers.
Recently the prostate Cancer risk management Programme (PCRMP) published updated guidance on prostate specific antigen (PSA) testing for primary care1 and the NHS screening committee has reviewed the evidence surrounding the utility of PSA screening.2 NICE published updated guidelines on the diagnosis and management of prostate cancer in 2014.3
PSA is a glycoprotein responsible for liquefying semen. It is expressed in both benign and malignant disorders that impact upon the integrity of the epithelial cells of the prostate. As the result of alterations in the architecture of PSA secreting prostatic glands in conditions such as prostatitis and benign prostatic enlargement (BPE), as well as prostate cancer, PSA is able to leak out, leading to increased levels in the bloodstream.
The PSA test clearly provides the opportunity for clinically relevant prostate cancer to be detected at a stage when treatment options are greater and outcomes may be improved. However, in some patients the PSA test may lead to investigations which can identify clinically insignificant cancers which would not have become evident in a man’s lifetime. Nowadays however, these cases are managed by active surveillance. In addition, a raised PSA may often indicate BPE, and this may provide an opportunity for treatment of this condition before complications develop.
There are both advantages and disadvantages for men of having a PSA test (see box 1), and these should be clearly explained to patients before the test is requested.
Other biomarkers
Recent research has been focused on identifying biomarkers to improve stratification of men with low-risk versus high-risk aggressive disease, so that men can be managed appropriately, minimising the potential harm of overdiagnosis and overtreatment.4,5
There are two promising urinary RNA biomarkers, prostate cancer antigen 3 (PCA3) and fusion gene TMPRSS2:ERG, both of which aim to distinguish between men with low-risk (indolent) and those with aggressive (clinically significant) cancers.6
PCA3 is highly overexpressed in more than 95% of prostate cancers, or up to 100 times greater in men with cancer than in those with a normal prostate.7,8
A systematic review found that the sensitivity of the PCA3 test (54-82%) was found to be less than PSA testing (81-98%) but the specificity for PCA3 was much better than for PSA (66-89% vs 5-28%).9 Potentially, the higher specificity would reduce overdiagnosis and overtreatment of lower risk cases.
A weakness of these studies was that none of them used PCA3 scores as a screening test to indicate the need for prostate biopsy, making it difficult to interpret its clinical value. However, PCA3 has also been considered as a reflex test for diagnosing prostate cancer in men who have already had a prostate biopsy, and found to be useful in reducing the rebiopsy rate.10
Prostate gene fusion between TMPRSS2 and ERG, an ETS (e-twenty-six) transcription factor is also overexpressed in about 50% of prostate cancers from PSA-screened cohorts.11,12 However, population-based cohorts have shown a much lower prevalence of 15%.12
The reasons for these differences in prevalence are not well understood, but the prevalence of TMPRSS2:ERG was found to be lowest in men with early stage tumours (T1), suggesting this marker may be useful in identifying men who harbour more aggressive disease.
Further research is still needed to understand fully its clinical utility in screening and its potential use in prostate cancer management as well as its prognostic utility.
Improving detection of early disease
False-negative rates with standard TRUS-guided biopsy can be as high as 45%.13 Up to half of men who are initially diagnosed with low-risk disease are under-staged and actually have a higher burden of high-risk disease. However, the utilisation of multiparametric MRI (mp-MRI) before prostate biopsy has the potential to improve the accuracy of the diagnosis and staging of prostate cancer. Lesions seen on a pre-biopsy mp-MRI can be used to select appropriate targets for TRUS or template biopsy, and may add additional information that can help decide what treatment should be used to manage patients with low- and intermediate-risk disease.14,15
Triage of men with clinical suspicion of prostate cancer (elevated PSA and abnormal DRE) to mp-MRI prior to prostate biopsy could increase the detection of men with clinically significant cancer that is likely to require treatment. This strategy could reduce the number of men with clinically insignificant disease who undergo unnecessary biopsy and treatment.
This would also reduce the rate of biopsy-related complications, including infections, which occasionally can be severe.16,17
The use of the transperineal as opposed to the transrectal route for biopsy can also reduce the risk of infection.
NICE guidelines3 currently recommend that men whose biopsies are negative on TRUS 10 to 12 cores biopsy should be further evaluated with mp-MRI.
If the man is negative on mp-MRI, then another biopsy should not be recommended unless there are other significant risk factors. Current evidence suggests this strategy will reduce the number and frequency of repeat biopsies required compared with routine systematic TRUS re-biopsy, and more information on this, and on the utility of mp-MRI, should soon to be available from the PROMIS trial which is due to report later this year.18
Treatment options for localised disease
NICE has published guidance on the various treatment options for localised prostate cancer.3 Evidence suggests that any benefit to a man from undergoing radical treatment for prostate cancer is likely to be maximal for those whose comorbidities and age suggest a life expectancy of more than ten years. Men with advanced prostate cancers are less likely to benefit from radical treatment alone.
Active surveillance and active monitoring
During active surveillance or monitoring the patient is followed up regularly by an oncologist or urologist. This option is offered to men who are generally younger and fitter and who wish to avoid the possibility of unnecessary treatment of indolent cancers.
The downside is that potentially disease may spread locally and advanced disease may develop which may be more difficult to treat.
The aim is to monitor those with stable disease and identify where radical treatment may be appropriate for those whose cancer progresses. Men on active monitoring will be monitored by serial PSA tests. Men on active surveillance will be monitored by serial PSA tests, mp-MRI and repeat prostate biopsies. Radical treatment with curative intent is offered if there are signs of disease progression.19
Radical prostatectomy (open, laparoscopic and robotic)
The aim of radical prostatectomy is to remove the entire prostate gland and thereby cure the disease. Complete tumour excision is not always achieved and approximately 20% of men go on to develop biochemical or clinical recurrence of the disease. Recurrence does not necessarily equate with death from prostate cancer, as second-line treatment with radiotherapy is an option. Complications of surgery include sexual dysfunction and stress urinary incontinence.
A study in the BMJ in 2014 reported improved survival in patients treated with surgery compared with those treated by radiotherapy.20
Radiotherapy (external beam and brachytherapy)
Radiotherapy such as external beam radiotherapy (EBRT) and brachytherapy also aims to cure the disease. EBRT involves an external source of radiation targeted at the tumour.
Short-term side-effects relate mainly to bowel and bladder problems from the radiation. Longer-term complications include sexual dysfunction and urinary problems as well as a significantly increased risk of secondary cancers in the pelvis. This treatment is not usually recommended for men with less than ten years’ life expectancy.
Brachytherapy may be given by two very different techniques. Low dose rate (LDR) brachytherapy involves the permanent implantation of tiny radioactive seeds into the prostate to deliver a high radiation dose into the gland.
High dose rate (HDR) brachytherapy requires fine catheters to be inserted into the prostate, through which a radioactive source is temporarily passed. Although the isotope used has a higher dose rate, the overall dose is lower than that given by LDR brachytherapy, so it is usually given in conjunction with EBRT. This latter technique is much more recent, with limited clinical data, and is usually reserved for patients with high-risk disease. Possible side-effects include urinary symptoms and sexual dysfunction.
Brachytherapy is best avoided in men with pre-existing lower urinary tract symptoms and bladder outflow obstruction as it may precipitate acute urinary retention.
High-intensity focused ultrasound and cryotherapy
High-intensity focused ultrasound (HIFU) and cryotherapy are newer radical therapies for the treatment of localised prostate cancer and are not currently recommended other than in the context of controlled clinical trials. HIFU aims to cure the disease by heating the prostate gland using ultrasound waves to cause tissue damage by mechanical and thermal effects as well as by cavitation. Cryotherapy aims to cure the disease by freezing the prostate gland.
Quality of life
Before choosing a treatment regimen, it is important that men should be appropriately counselled about the important quality of life differences between the options.
Both surgery and radiotherapy aim to extend life by curing the cancer. However, there is a trade off as surgical removal of the prostate can result in loss of erectile function, ejaculation, fertility, and urinary continence. Radiotherapy is associated with persisting lower bowel disturbance and an increased incidence of secondary malignancies.
Active surveillance may result in increased anxiety and the psychological stress of a cancer diagnosis.
Monitoring and follow-up
The lack of sensitivity and specificity that characterises PSA testing in the initial diagnosis of prostate cancer largely disappears after treatment of localised prostate cancer, especially after surgery. Three monthly PSA measurement is usually recommended for the first year after primary treatment. Subsequently less frequent testing is required.
A PSA rise after primary treatment usually indicates biochemical recurrence and often the need for further therapy.
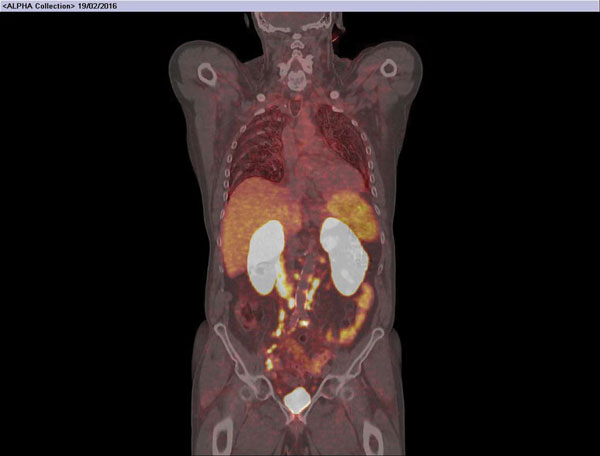
In this context it has often been difficult to determine the exact location of the recurrence, but recently the availability of PMSA PET CT scanning has helped differentiate between disease recurrence in the prostate bed, lymph nodes or bones, see figures 1 and 2. This information can facilitate the selection of second-line treatment, including hormone therapy or radiotherapy.
Conclusions
The debate about the benefits and potential risks of PSA testing seems certain to continue. The two major studies of PSA as a screening test for prostate cancer did not utilise mp-MRI in advance of the biopsy to target the lesion and select out those men with higher risk disease who are more likely to benefit from treatment.21,22 Had they done so it seems likely that a greater benefit would have been seen, and the risk of overtreatment of men with clinically insignificant disease would have been greatly reduced.
In any case, nowadays, men with low volume, low-risk, Gleason pattern 3+3=6 cancers are nearly all managed initially by active surveillance, at least in the first instance, so the consequences of overdiagnosis are very much less significant.3
Current guidance from the PCRMP recommends that GPs refer informed men between the ages of 50 and 69 with a PSA value ≥ 3.0 ng/ml for further assessment including possible mp-MRI and biopsy, see figure 3.23
After initial treatment, PSA testing at regular intervals during follow-up is of considerable value, as a rising PSA usually indicates a recurrence and second-line therapy can then be deployed.
REFERENCES
1 www.gov.uk/guidance/prostate-cancer-risk-management-programme-overview
2 UK National Screening Committee. The UK NSC recommendation on prostate cancer screening/PSA testing in men over the age of 50. 2016. http://legacy.screening.nhs.uk/prostatecancer
3 National Institute for Health and Care Excellence CG175. Prostate cancer: diagnosis and treatment. NICE. London. 2014
4 Cuzick J, Thorat MA, Andriole G et al. Prevention and early detection of prostate cancer. Lancet Oncol 2014;15(11):e484-e92
5 Truong M, Yang B, Jarrard DF. Toward the detection of prostate cancer in urine: a critical analysis. J Urol 2013;189(2):422-9
6 Bussemakers MJ, van Bokhoven A, Verhaegh GW et al. DD3: a new prostate-specific gene, highly overexpressed in prostate cancer. Cancer Res 1999;59(23):59757-9
7 De Kok JB, Verhaegh GW, Roelofs RW et al. DD3(PCA3), a very sensitive and specific marker to detect prostate tumors. Cancer Res 2002;62(9): 2695-8
8 Vlaeminck-Guillem V, Ruffion A, Andre J et al. Urinary prostate cancer 3 test: toward the age of reason? Urology 2010;75(2):447-53
9 Nicholson A, Mahon J, Boland A et al. The clinical effectiveness and cost-effectiveness of the PROGENSA(R) prostate cancer antigen 3 assay and the Prostate Health Index in the diagnosis of prostate cancer: a systematic review and economic evaluation. Health Technol Assess 2015;19(87):1-192
10 Kirby RS and Fitzpatrick JM. Optimising repeat prostate biopsy decisions and procedures. BJU Int 2012; 109(12):1750-4
11 Kumar-Sinha C, Tomlins SA, Chinnaiyan AM. Recurrent gene fusions in prostate cancer. Nature Reviews Cancer 2008;8(7):497-511
12 Tomlins SA, Rhodes DR, Perner S et al. Recurrent fusion of TMPRSS2 and ETS transcription factor genes in prostate cancer. Science 2005;310(5748):644-48
13 Djavan B, Ravery V, Zlotta A et al. Prospective evaluation of prostate cancer detected on biopsies 1, 2, 3 and 4: when should we stop? J Urol 2001;166(5):1679-83
14 Turkbey B, Pinto PA, Mani H et al. Prostate cancer: value of multiparametric MR imaging at 3 T for detection–histopathologic correlation. Radiology 2010;255(1):89-99
15 Dickinson L, Ahmed HU, Allen C et al. Magnetic resonance imaging for the detection, localisation, and characterisation of prostate cancer: recommendations from a European consensus meeting. Eur Urol 2011;59:477-94
16 Challacombe B, Dasgupta P, Patel U et al. Recognizing and managing the complications of prostate biopsy. BJU Int 2011;108(8):1233-4
17 Patel U, Dasgupta P, Amoroso P et al. Infection after transrectal ultrasonography-guided prostate biopsy: Increased relative risks after recent international travel or antibiotic use. BJU Int 2012;109:1781-85
18 El-Shater Bosaily A, Parker C, Brown LC et al. PROMIS - Prostate MR imaging study: A paired validating cohort study evaluating the role of multi-parametric MRI in men with clinical suspicion of prostate cancer. Contemp Clin Trials 2015;42:26-40
19 Klotz L, Vesprini D, Sethukavalan P et al. Long-term follow-up of a large active surveillance cohort of patients with prostate cancer. J Clin Oncol 2015;33(3):272-77
20 Sooriakumaran P, Nyberg T, Akre O. Comparative effectiveness of radical prostatectomy and radiotherapy in prostate cancer: observational study of mortality outcomes. BMJ 2014;348:g1502
21 Andriole GL, Crawford ED, Grubb RL 3rd et al. Prostate cancer screening in the randomized Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial: mortality results after 13 years of follow-up. J Natl Cancer Inst 2012;104(2):125-32
22 Schroder FH, Hugosson J, Roobol MJ et al. Screening and prostate cancer mortality: results of the European Randomised Study of Screening for Prostate Cancer (ERSPC) at 13 years of follow-up. Lancet 2014;384 (9959):2027-35
ARTICLE IN PDF

PRESET SEARCHES
NICE- evidence search results
Prostate cancer
Metastatic
UK key resources
Risk management programme overview
PubMed
PubMed is a database of the US National Library of Medicine/National Institutes of Health
Benign prostatic hyperplasia and prostate cancer
BPH relation to prostate cancer
US: National Cancer Institute
PDQ® (Physician Data Query) is NCI's cancer database of peer-reviewed, regularly updated evidence-based, referenced summaries
Prostate prevention
Prostate screening
Prostate treatment
Cancer Research UK
Prostate cancer statistics
EXTERNAL WEBLINKS
We welcome your feedback
If you would like to comment on this article or have a question for the author, write to: [email protected]
Useful information